Featured Article:Melatonin and Sleep Disorders: The Neurobiology of Sleep, Circadian Rhythm Sleep Disorders, and Various Treatment Methods
By
2013, Vol. 5 No. 07 | pg. 3/3 | « Circadian Rhythm Sleep Disorders3.1 Definition and Introduction The term ‘circadian rhythm sleep disorder’ (CRSD) is used to describe a host of chronic conditions in which there is a misalignment between the individual’s normal circadian sleep rhythm and the external, environmental day-night/dark-light cycle (Zisapel, 2010). Sleep is normal but its timing is not. Therefore, one is unable to sleep during the desired day hours and is awake at inappropriate times with resultant social, economic and mental consequences. There are 6 main types of CRSDs and they can be divided into 2 categories. Intrinsic CRSDs are due to some malfunction of the internal circadian rhythm whereas extrinsic CRSDs stem from imposed alterations to the usual sleep-wake behavior. Moreover, the International Classification of Sleep Disorders has also acknowledged other CRSDs attributable to substance abuse, depression, stroke and head injury as well as other non-specified causes (Drake, 2010). 3.2 Pathophysiology of Circadian Rhythm Sleep DisordersThe pathophysiological processes that characterize CRSDs are thought to be associated with either pacemaker abnormalities, inability of synchronization to external cues or malfunctions of the downstream regulating mechanisms (Zisapel, 2010). 10% of complaints of insomnia are accredited to Delayed Sleep Phase Syndrome making this condition the commonest CRSD. Usually patients are teenagers who are unable to sleep before a given time, characteristically sleeping and waking late with sleep initiation reportedly difficult, if outside preferred sleep time. The atypical sleep onset and offset times they experience are due to dysfunction of the SCN, more specifically Per3 gene polymorphisms. Approximately 40% of individuals presenting with Delayed Sleep Phase Syndrome have a family history of the disorder (Martinez and Lenz, 2010; El Shakankiry, 2011). Conversely, in Advanced Sleep Phase Disorder, patients sleep and wake early, reporting somnolence in the late afternoon. Population prevalence is about 1%, commonly in the middle-aged and elderly. Both environmental and genetic factors are implicated in ASPD. In fact, it was the first CRSD to have its mendelian pattern of inheritance defined (Sharma and Feinsilver, 2009; Martinez and Lenz, 2010). In families with this disorder, the binding region of the gene hPER2, known as casein kinase 1, is mutated due to an amino acid substitution from serine to glycine (Toh et al., 2001). Irregular sleep-wake rhythm is a type of CRSD characterized by erratic sleep-wake patterns even though total sleep duration is normal. Its prevalence increases with age. Predisposing factors include poor sleep hygiene and lack of external agents capable of synchronising the circadian timekeeper. Examples of such agents would be sunlight and social activities. A rare CRSD known as Non 24-hour sleep-wake syndrome or Non-entrained type, has been reported mostly in the blind; about 50% of blind individuals experience NET. The lack of external light-dark signals is the cause of the disorder. This results in the free-running of the patient’s circadian rhythm causing it to mimic the SCN’s intrinsic one which is somewhat longer than 24 hours (Sharma and Feinsilver, 2009; Martinez and Lenz, 2010). The two extrinsic CRSDs are Shift Work Sleep Disorder (SWSD) and Time Zone Change Syndrome otherwise known as jet lag. The former is estimated to be prevalent in around 2-5% of the population working irregular hours and higher in females. It is associated with the development of hypertension and cancer of the female reproductive system. Alertness, along with work performance, is decreased which causes an increased risk of work-related errors and accidents. SWSD pathophysiology involves the inability of the individual to entrain their circadian rhythm to their new sleep schedule. Melatonin production and consequently patterns of sleep are altered. Jet lag is generally experienced after travel across two or more time zones and starts a couple of days after arrival. It is brought about by a temporary discrepancy in one’s endogenous circadian rhythm in relation to time in the destination country. The extent of severity of symptoms depends according to number of time zones crossed and trip direction. For instance, if one travels eastward, sleep will be phase-delayed and symptoms more severe. In addition, children tend to cope better than adults. Spontaneous resolution typically occurs within a week (Sharma and Feinsilver, 2009; Martinez and Lenz, 2010; El Shakankiry, 2011). TABLE 3.1: Summary of Circadian Rhythm Sleep Disorders (reproduced from Abbas et al., 2010)
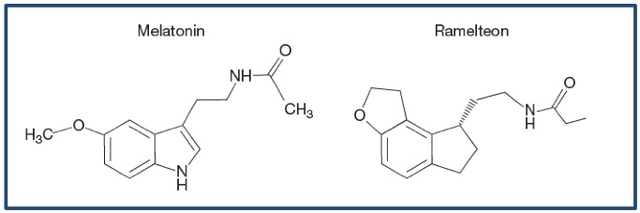
3.3 Implications of melatonin’s chronobiotic actions in CRSDs Given the close relation between endogenous melatonin secretion and sleep-wake cycle regulation, melatonin can theoretically be manipulated to influence the sleep-wake cycle. It has been, in fact, successfully used therapeutically for insomnia and other circadian rhythm sleep disorders. It was shown on patients suffering from Delayed Sleep Phase Syndrome that 5 mg of melatonin administered for four weeks 5 hours prior to onset of sleep induces phase-advancement (Cajochen et al., 2003). In addition, melatonin was also used to try and decrease the effects of jet lag, after at least 5 time zones were crossed. In 9 out of 10 trials results proved to be positive even though safety, optimum dosage and timing of ingestion still need to be defined (Herxheimer and Petrie, 2002; Zisapel 2010). Currently, melatonin seems to be the only drug for blind patients with NET. It is possibly one of the better approaches to sleep disorders because it not only treats the sleep-wake problems but also entrains body rhythms maintaining a synchronised internal milieu (Zisapel, 2010). Treatment and Pharmacological Directions in the Management of Circadian Rhythm Sleep Disorders4.1 Introduction Melatonin, despite its chronobiotic actions, has a short half-life which prevents it from exerting its effects fully. Furthermore, it has not been approved by the US Food and Drug Association. Its status as a food supplement makes it nonpatentable thereby deterring the pharmaceutical industry from paying attention to its direct use in the treatment of sleep disorders (Pandi-Perumal et al., 2007). This section will strive to acquaint the reader with the current drugs available for the management of sleep disorders related to circadian rhythm disruptions. 4.2 Current Pharmacological Therapy Circadin ® To circumvent the problem of melatonin’s half-life, Circadin® also known as PRM – prolonged release melatonin – was designed. Melatonin blood profile, after evening ingestion, was shown to be comparable to normal physiological levels. PRM seems to exhibit benefits related to sleep promotion, sleep quality and increased morning alertness. In July 2007, it was authorised by the European Commission as short-term treatment for patients, aged 55 or over, suffering from primary insomnia. PRMS’s efficacy is probably due to its physiological influence as a circadian clock synchronizer. Its unique effect of increased morning alertness suggests that non-MT1/MT2 pathways are involved and thus, further studies are necessary so as to determine its mechanism of action (Zisapel, 2010). Agomelatine and Tasimelteon Agomelatine (S20098), a novel melatonergic antidepressant, acts as a selective antagonist to serotonin receptors. However, being also an agonist of MT1 and MT2 receptors, it can affect sleep architecture, efficiency and duration. Its oral absorption is rapid and hepatic metabolism occurs mainly by three cytochrome P450 isoenzymes. Agomelatine’s half-life is approximately 2 hours (Srinivasan et al., 2011). Tasimelteon (VEC-162) is another melatonin receptor agonist which is thought to provide effective treatment for CRSDs. Preclinical studies on tasimelteon have shown that it parallels melatonin’s phase-shifting actions. Vasoconstriction side-effects are not as significant (Vachharajani et al., 2003). Detailed pharmacokinetic data of Tasimelteon on humans is yet to be disclosed (Hardeland, 2009). Ramelteon The most widely described drug in the literature that acts as a melatonin analog is Ramelteon, approved for the treatment of insomnia by the FDA in 2005. This synthetic drug’s actual chemical name is N-{2-[(8S)-1,6,7,8-tetrahydro-2H-indeno[5,4-b]furan-8-yl]ethyl}propanamide and has a molecular weight of 259.34 Da. Ramalteon has a very high specificity for both MT1 and MT2 receptors. Specificity for the former transpires to be more than 1000-fold than that for the MT2 receptors and the drug has no other relevant affinity for serotonin, opiate, benzodiazepine and dopamine binding receptors (Miyamoto et al., 2004; Srinivasan et al., 2011). Ramelteon’s pharmacokinetics and pharmacodynamics depend on age but not on gender; in fact, clearance decreases in the elderly thereby increasing half-life. Administration is usually oral and absorption rapid. Absolute bioavailability however is approximately only 1.8% due to a significant first-pass effect. Hepatic metabolism is primarily mediated by cytochrome P450 1A2, therefore CYP1A2 inhibitors can theoretically increase ramelteon levels. Four ramelteon metabolites have been distinguished. When compared to melatonin, lipophilicity and subsequent tissue absorption is greater; affinity for MT1 and MT2 receptors is also greater with ramelteon. Also, having a longer half-life aids its efficiency in promoting sleep (Pandi-Perumal et al., 2007; Srinivasan et al., 2011). In an animal model involving cats, ramelteon was found to decrease wakefulness and enhance slow-wave sleep. In rats, it appeared to be useful in the re-entrainment of their circadian rhythms even though its action as a chronobiotic is still dubious. Its dependence potential, by interaction with other CNS areas such as opioid binding sites, was ruled out in a different study on a particular monkey species. This specificity is why it does not have a significant side effect profile. In three clinical studies of which one was randomized, double-blind and placebo-controlled, a reduction in sleep latency and an increase in total sleep time was noted. The former could be due to ramelteon’s capability of affecting the sleep-wake ‘flip-flop’ switch mentioned previously and thus hasten the onset of sleep via SCN receptors. Infrequent but severe adverse effects of ramelteon include galactorrhea, amenorrhea, nausea and depression. Intense fatigue and decreased libido have also been reported. More common side-effects comprise sore throat and headache (Pandi-Perumal et al., 2007). Figure 4.1: The chemical structures of melatonin and ramelteon.
4.4 What the Future Holds One of the major questions that can only be answered by future scientific investigation is whether ramelteon is safe for long-term treatment and safe for the elderly. Toxicology tests for ramelteon, tasimelteon and agomelatine also need to be carried out. It appears that melatonin agonists could also prove to be useful in the treatment of other disorders such as Smith-Magenis Syndrome and chronic obstructive pulmonary disorder (Hardeland, 2009). The impact of CRSDs on health and lifestyle seems to be underestimated. The potential that melatonin agonists therefore hold in the pharmacological industry is considerable. Development of such chronobiotic drugs depends on progress in the better understanding of sleep physiology and its genetic influences. Enhanced collaboration between basic science researchers and sleep medicine clinicians should aid new discoveries and result in better treatment (Mahowald and Schenck, 2005; Sharma and Feinsilver, 2009; Dodson and Zee, 2010). ReferencesAbbas, A., Raju, J., Milles, J. and Ramachandran, S. (2010) A circadian rhythm sleep disorder: melatonin resets the biological clock. J R Coll Physicians Edinb, 40, 311-313. Albrecht, U. (2012) Circadian Rhythms and Sleep – the Metabolic Connection. Eur J Physiol, 463, 23-30. DOI: 10.1007/s00424-011-0986-6. Arendt, J. (1998) Melatonin and the pineal gland: influence on mammalian seasonal and circadian physiology. J Reprod Fertil, 3, 13-22. Arendt, J., Van Someren, E.J.W., Appleton, R., Skene, D.J. and Akerstedt, T. (2008) Clinical update: melatonin and sleep disorders. Clin Med, 8, 381-383. Arendt, J. and Rajaratnam, S.M.W. (2008) Melatonin and its agonists: an update. BJ Psych, 193, 267-269. DOI: 10.1192/bjp.bp.108.050955 Barrenetxe,J., Delagrange,P. and Martinez, J.A. (2004) Physiological and metabolic functions of melatonin. J Physiol Biochem, 60, 61-72. Cajochen, C., Krauchi, K. and Wirz-Justice, A. (2003) Role of melatonin in the regulation of human circadian rhythms and sleep. J Neuroendocrinol, 15, 432-437. Carlberg, C. and Weisenberg, I. (1995) The orphan receptor family RZR/ROR, melatonin and 5-lipoxygenase: an unexpected relationship. J Pineal Res, 18, 171-178. Claustrat, A., Brun, J. and Chazot, G. (2005) The basic physiology and pathophysiology of melatonin. Sleep Medicine Reviews, 9, 11-24. Dodson, E.R. and Zee, P.C. (2010) Therapeutics for Circadian Rhythm Sleep Disorders. Sleep Med Clin, 5, 701-715. Drake, C.L. (2010) The characterization and pathology of circadian rhythm sleep disorders. J Fam Pract, 59, 1(Suppl.) 12-17. Dubocovich, M.L. and Markowska, M. (2005) Functional MT1 and MT2 receptors in mammals. Endocrine, 27, 101-110. El Shakankiry, H.M. (2011) Sleep physiology and sleep disorders in childhood. Nature and Science of Sleep, 3, 101-114. Facciola, G., Hidestrand, M., von Bahr, C. and Tybring, G., (2001) Cytochrome P450 isoforms involved in melatonin metabolism in human liver microsomes. Eur J Clin Pharmacol, 56, 881-888. Foster, C.E., Bianchet, M.A., Talalay, P., Faig, M. and Amzel, L.M. (2000) Structures of mammalian cytosolic quinone reductases. Free Radic Biol Med, 29, 241-245. Fournier, I., Ploye, F., Cottet-Emard, J.M., et al. (2002) Folate deficiency alters melatonin secretion in rats. J Nutr, 132, 2781-2784. Fourtillan, J.B., Brisson, A.M, Gobin, P., Ingrand, I., Decourt, J.P. and Girault, J. (2000) Bioavailability of melatonin in humans after day-time administration of D(7) melatonin. Biopharm Drug Dispos, 21, 15-22. Grace, M.S., Cahill, G.M. and Besharse, J.C. (1991) Melatonin deacetylation: retinal vertebrate class distribution and Xenopus laevis tissue distribution. Brain Res, 559, 56-63. Hardeland, R. (2009) New approaches in the management of insomnia: weighing the advantages of prolonged-release melatonin and synthetic melatoninergic agonists. Neuropsychiatric Disease and Treatment, 5, 341-354. Herxheimer, A. and Petrie, K.J. (2002) Melatonin for the prevention and treatment of jet lag. The Cochrane Database Syst Rev,CD001520. Lockley, S.W., Skene, D.J., Tabandeh, H., Bird, A.C., Defrance, R. and Arendt, J. (1997) Relationship between napping and melatonin in the blind. J. Biol. Rhythms, 12, 657-665. Luboshitzky, R., Ophir, U., Nave, R., et al. (2002) The effect of pyridoxine administration on melatonin secretion in normal men. Neuroendocrinol Lett, 23, 213-217. Mahowald, M.W. and Schenck, C.H. (2005) Insights from studying human sleep disorders. Nature Insight Review, 437, 1279-1285. Martinez, D. and do Carmo Sfreddo Lenz, M. (2010) Circadian rhythm sleep disorders. Indian J Med Res, 131, 141-149. Miyamoto, M., Nishikawa, H., Doken, Y., Hirai, K, Uchikawa, O. and Ohkawa, S. (2004) The sleep promoting action of ramelteon (TAK-375) in freely moving cats. Sleep, 27, 1319-1325. Munoz-Hoyos, A., Amoros-Rodriguez, I., Molina-Carballo, A., et al. (1996) Pineal response after pyridoxine test in children. J Neural Transm Gen Sect, 103, 833-842. Pace-Shott, E.F. and Allan Hobson, J. (2002) The neurobiology of sleep: genetics, cellular physiology and subcortical networks. Nature, 3, 591-605. Pandi-Perumal, S.R., Srinivasan, V., Maestroni, G.J.M., Cardinali, D.P., Poeggeler, B. and Hardeland, R. (2006) Melatonin- Nature’s most versatile biological signal? FEBS J, 273, 2813-2838. Pandi-Perumal, S.R., Srinivasan, V., Poeggeler, B., Hardeland, R. and Cardinali, D.P. (2007) Drug Insight: the use of melatonergic agonists for the treatment of insomnia – focus on ramelteon. Nature Clinical Practice, Neurology, 3, 221-228. Pandi-Perumal, S.R., Trakht, I., Brown, G.M. and Cardinali, D.P. (2008) Melatonin, Circadian Dysregulation and Sleep in Mental Disorders. Primary Psychiatry, 15, 77-82. Purves, D., Augustine, G.J., Fitzpatrick, D., Hall, W.C., et al. (2008) Neuroscience 4th ed. Sinauer Associates, Inc., Massachusetts. (ISBN: 978-0-87893-697-7) Rajaratnam, S.M., Middleton, B., Stone, B.M., Arendt, J., and Dijk, D.J. (2004) Melatonin advances the circadian timing of EEG sleep and directly facilitates sleep without altering its duration in extended sleep opportunities in humans. J Physiol, 561, 339-351. Saper, C.B., Scammell, T.E. and Lu, J. (2005) Hypothalamic regulation of sleep and circadian rhythms. Nature, 437, 1257-1263. Schwartz, J.R.L. and Roth, T. (2008) Neurophysiology of Sleep and Wakefulness: Basic Science and Clinical Implications. Curr Neuropharmacol, 6, 367-378. Sharma, B. and Feinsilver, S. (2009) Circadian rhythm sleep disorders: An update. Sleep and Biological Rhythms, 7, 113-124. Shochat, T., Haimov, I., Lavie, P. (1998) Melatonin – the key to the gate of sleep. Ann Med, 30, 109-114. Sletten, T.L., Vincenzi, S., Redman, J.R., Lockley, S.W. and Rajaratnam, S.M.W. (2010) Timing of sleep and its relationship with the endogenous melatonin rhythm. Front Neurol, 1, 137. DOI:10.3389/fneur.2010.00137 Srinivasan, V., Cardinali, D.P., Pandi-Perumal, S.R. and Brown, G.M. (2011) Melatonin agonists for treatment of sleep and depressive disorders. J Exp Integr Med, 1, 149-158. Toh, K.L., Jones, C.R., He, Y. et al. (2001) An hPer2 phosphorylation site mutation in familial advanced sleep phase syndrome. Science, 291, 1040-1043. Vachharajani, N.N., Yeleswaram, K. and Boulton, D.W. (2003) Preclinical pharmacokinetics and metabolism of BMS-214778, a novel melatonin receptor agonist. J Pharm Sci, 92, 760–72. Zawilska, J.B. , Skene, D.J. and Arendt, J. (2009) Physiology and pharmacology of melatonin in relation to biological rhythms. Pharmacol Rep, 61, 383-410. Zimmermann, R.C., McDougle, C.J., Schumacher, M., et al. (1993) Effects of acute tryptophan depletion on nocturnal melatonin secretion in humans. J Clin Endocrinol Metab, 76, 1160-1164. Zisapel, N. (2000) Development of a melatonin based formulation for the treatment of insomnia. Drug Dev Re, 50, 226-234. Zisapel, N. (2010) Melatonin and sleep. The Open Neuroendocrinology Journal, 3, 85-95. Figure 1.1a - Online: The PubChem Project (2009) – Melatonin Compound Summary, National Centre for Biological Information. Retrieved from: http://pubchem.ncbi.nlm.nih.gov/summary/summary.cgi?cid=896 [Accessed: 22/12/2011] Figure 1.1b – Online: Melatonin Information Source (2006) – Molecular Structure. Retrieved from: http://www.melatoninsource.co.uk/page2.html [Accessed: 23/03/2012] List of Abbreviations5-HT : 5-hydroxytryptophan CRSD : circadian rhythm sleep disorder NET : non-entrained type PRM : prolonged release melatonin NAT : serotonin N-acetyl transferase SCN : suprachiasmatic nucleus SWSD : shift work sleep disorder VLPO : ventrolateral preoptic nucleus
KEYWORDS:

From the Inquiries Journal Blog   Monthly Newsletter SignupThe newsletter highlights recent selections from the journal and useful tips from our blog. Suggested Reading from Inquiries Journal
Inquiries Journal provides undergraduate and graduate students around the world a platform for the wide dissemination of academic work over a range of core disciplines. Representing the work of students from hundreds of institutions around the globe, Inquiries Journal's large database of academic articles is completely free. Learn more | Blog | Submit Follow IJ
Latest in Health Science |