Cancer Epidemiology in Romani-Americans: A Review of the Current Literature
By
2021, Vol. 13 No. 10 | pg. 1/1
IN THIS ARTICLE
KEYWORDS
AbstractRomanies are one of history’s most misunderstood ethnic populations. Since medieval times, they have faced slavery, forced assimilation, sterilization, genocide, and other forms of ethnic cleansing. Their cultural and historical persecution has led to adverse health outcomes. Studies on health inequality among Romanies have been conducted in the past, as well as fragmented research on their genetic predisposition to disease; however, there is a gap in available information regarding precancerous health risks, especially at the upstream, social end of the spectrum. Thus, their oppression is largely unacknowledged. This holds true in the United States where their numbers are far smaller than the majority who live in Eastern Europe. Ignorance of their history and culture breeds stigma, erecting a barrier to positive health outcomes for Romani-Americans. The primary objective of this study is to analyze the biological, cultural, and socioeconomic factors leading to cancer and other chronic disease in Romani-Americans through a review of the existing literature. I point out the most prominent causes of chronic disease as a proxy to cancer in Romani-Americans; I also hope to draw attention to the lack of research in the field and inspire others to pursue such research. IntroductionThe Romanies—otherwise known as the Roma, and sometimes erroneously called “gypsies”—are an ancient ethnic group with origins in North India. Though the majority live in Eastern Europe, through the slave trade and waves of immigration before and after the two world wars, a number of them have made their way to the United States of America. Throughout American history, Romanies have been misrepresented in popular culture and media. For example, the weddings of some wealthy Romani-Americans are displayed in the television series “My Big Fat American Gypsy Wedding.” Unfortunately, the television series is a poor representation of Romani culture and values. With the show’s stars shunning an education, sexualizing their children, and the program’s conflation of Romanies with Irish Travelers (an entirely different group of people), not only is it insulting to many in the Roma community, but it also negatively portrays this ethnic group to other Americans who watch the show.Not many Americans know that “gypsy” is a racial slur. The use of “gypsy” is rarely intended to be harmful; Americans simply are unaware that this is a real group of people. In their hit song “Nothin’ Like You,” country-pop duo Dan + Shay sings about stealing a woman’ heart “like a gypsy.” What is more troubling is the word “gypped,” which is commonly used in English language to refer to stealing. This word comes from an age-old distrust of Romanies, and is hurtful and racist because it attaches a negative stereotype of dishonesty and thievery to the group. Such negative stereotypes lead to their oppression. This lack of awareness of Romanies causes a host of problems. One of these is that there is not enough healthcare work being done for the Romani people, especially for Romani-Americans. In my research, I have found surprisingly few recent studies on chronic disease and health of American Romanies. Others have faced the same struggle—Hajioff & McKee’s “The health of the Roma people: a review of the published literature” shows that only 8 of the 110 publications on Romani health found were based in the United States (Hajioff & McKee, 2000). This lack of accessible information makes it hard for interested scholars to learn and for any policy changes and activism to take place. So long as Americans remain ignorant of the existence of Romanies and the struggles they face, they will continue to suffer from treatment as second-class citizens, just as they currently do throughout Europe. This ignorance also makes it difficult for cultural sensitivity to take place in interactions with non-Romanies—whom Romanies refer to as gadje—especially in healthcare. For example, Romanies have strict standards regarding purity (wuzho), which lead to misunderstandings with healthcare providers in the hospital setting. Structural competency in healthcare is critical today because health outcomes are becoming increasingly dependent on the severity of upstream public health risks. As American society makes its transition into what epidemiologist Dr. Abdel Omran calls “The Age of Degenerative and Man-Made Diseases,” the incidence of communicable diseases declines, while noncommunicable disease rates climb (Omran, 2005). America once watched the likes of the bubonic plague, Spanish Flu, and tuberculosis claim lives—but thanks to strides in public health and our longer lifespans, we now mostly see people suffer from chronic diseases, including the one that was once considered an inevitable death sentence: cancer. Cancer, while famously called “the emperor of all maladies” by oncologist and writer Dr. Siddhartha Mukherjee, also acts as a proxy to chronic disease (Mukherjee, 2010). The mechanisms of the onset and progression of cancer can reveal the ways in which all of one’s life events—from lifestyle and stress levels to even genetic predisposition—influence how, when, and how severely the illness takes hold (Petrášová et al., 2014). For that reason, it is a comprehensive tool to measure health in a population. In fact, according to the Department of Health and Human Services (US) Centers for Disease Control and Prevention (CDC), cancer is the only chronic, non-infectious condition for which there is national data for incident cases because providers are required to report data to the state (White et al., 2017). Thus, its burden on public health can be measured at the local, state, and national levels, as well as by selected demographics. This work is a meta-analysis of information from a large variety of sources. Some of these will be clinical case studies, personal accounts, and biographies about prominent historical figures, whereas other information will be gathered from sources such as dictionaries of Romani language, since linguistics are an important way to understand Romani culture. I hope to accumulate data from a broad range of perspectives in order to approach epidemiology in these people from a different angle than others have before me. My experiences as a Romani-Hungarian immigrant living in the United States provide unique firsthand, insider knowledge that serves to enrich this discussion; there are not many existing genetic studies on Romanies that have been conducted by Romanies themselves. My hope is that my research will draw more attention to the issues faced by the Romani people. Learning about the factors that cause cancer and other chronic diseases in Romanies could bring much-needed awareness to what is perhaps one of the most disenfranchised ethnic groups in today’s world. By increasing awareness of the struggles of the Romanies, as well as addressing their misrepresentation in American media and popular culture, we can crumble the divide that prevents these people from receiving the high quality, structurally competent healthcare they deserve. BackgroundThere is simply not enough available information about healthcare in Romanies, especially in America. Systematic poverty and the consequent lack of education worsen Romani-Americans’ likelihood of engaging in high-risk, unhealthy behaviors such as excessive alcohol consumption and smoking; meanwhile, lack of access to electricity and clean water is part of the cause for the ethnic group’s high Hepatitis B and C rates (Sedláková, 2014). For Romani-Americans living off-grid—which are the majority of them—that is a problem. Lack of access to basic physiological needs is just one of the factors leading to the group’s high rates of chronic disease, including fatty liver disease, diabetes, cardiovascular disease, and—of course—cancer. I focus on cancer in particular because it is comorbid with a variety of chronic diseases, making it a valuable indicator of a population’s health. It provides an effective segue into discussion about upstream health issues, such as the poverty-related ones mentioned above, or national healthcare policies that affect the health outcomes of citizens. For the sake of my thesis, I define institutional racism as how racism is practiced at a systemic level, such as by the government, in schools, in access to housing, or in this case, in healthcare. The Intersection of History, Culture, and HealthHistory of the RomaniesBecause of the word “gypsy,” one might erroneously presume that the Romanies come from Egypt. In truth, though, the Romanies originate from India, specifically in North India. They began their migration from India at the beginning of the 11th century as a composite Indian people assembled to resist the eastward spread of the Ghaznavid Empire; they entered Europe 200-250 years later as a result of the westward expansion of the Ottoman Empire, and their movement brought them to the European continent around the 11th century (Hancock, 2010, 2016). Evidence that Romanies descended from Indian people can be found at the molecular level. Romanies share identical by descent (IBD) fragments at a rate of .132 Mb with Northwest Indians, specifically in the states of Punjab, Rajastha, and Gujarat. Additionally, a rate of .087 was found with Pakistani groups of Balochi, Brahui, Burusho, Kalash, Makrani, Pashtun, and Sindhi (Melegh et al., 2017). This is considered to be a significant IBD fragment detection rate; for comparison, the creators of the IBD scale conducted a sample study on 4899 random individuals in Northern Finland, excluding close relatives, and analyzed close to 300,000 autosomal single nucleotide polymorphisms (SNPs) (Browning, B. & Browning, S., 2013). The IBD rate was detected to be .015. A similar experiment was conducted by the same group on 5200 individuals from the United Kingdom, and analyzed close to 900,000 autosomal SNPs (Browning, B. & Browning, S., 2013). The IBD detection rate was .0041. It makes sense that the population from Northern Finland would have a higher IBD detection rate than the population from the entire UK, since the latter analyzes a population from a wider geographic range. The diaspora from North India took a variety of migratory routes. For example, some groups migrated on paths through the Caucasus region and Eurasia to reach what is today Europe; others—the majority, in fact—migrated to what was then the Ottoman Empire, choosing to live there because it was tolerant of a variety of ethnic groups (Martínez-Cruz et al., 2015). It is likely that this split caused both a bottleneck and later founder effects, which account for such genetic homogeneity within today’s Romani population. A genetic bottleneck is a biological phenomenon that defines a sharp decline in a species’ population—whether due to a natural disaster, disease, or social event (such as the Holocaust or other genocide). The Romanies also epitomize the founder effect because it occurs when a small segment of a group migrates, settles, and colonizes an area, leading to decreased genetic diversity in descending lineages. There are substantial genetic similarities between the Roma and Northern Indian peoples, and while looking at mitochondrial DNA and Y chromosome H haplogroups supports this, Martínez-Cruz et al. show that there are other founder lineages in today’s Romani population (Martínez-Cruz et al., 2015). Through the results of this study, it is possible to trace gene flow between the Roma and other ethnic populations, which can offer clues about where Romanies came from. The findings outlined in the article suggest that there was a bottleneck in addition to the founder effect that contributed to the genetic homogeneity within today’s Romanies. Not only is there evidence at the genetic level that Romanies came from North India; upon analysis and comparison of their immune systems with those of Europeans, there is also proof that Romanies evolved such that they are no longer genetically the same as the proto-Romanies who first migrated from North India. The immune systems of Romanies and Europeans evolved convergently due to the pathological profile of the region (Laayouni et al., 2014). Certain adaptive pressures, such as the plague, smallpox, and other epidemics, shaped their modern-day immune systems. One gene group illustrating this phenomenon is the Toll-like immune pathway TLR1/TLR6/TLR10, which reveals patterns shared between Europeans and Romanies, but not today’s North Indians. Laayouni et al. determined that Romanies and Europeans, though possessing different origins, evolved in parallel ways in response to the same infectious environment. Toll-like receptor signaling pathways are important in activating the innate immune system against pathogens, and thus can serve as targets in cancer immunotherapy. Understanding how this key gene group has evolved over time in Romanies (and how this compares with the same genes in other Europeans) is an effective way to understand the selection pressures that shaped special genetic traits in Romanies, and how these traits contribute to their health today. Of the ancient proto-Romanies who decided to move to Europe instead of the Ottoman Empire, two of the smaller groups that continued to migrate throughout the continent were the most prominent: the Vlax Roma and the Romungro. Martínez-Cruz et al. describe how the Vlax Roma descended from the original migrants who moved from the east to across the Danube River around modern-day Romania, Moldova, and Hungary; the Romungro, on the other hand, spread into the Austro-Hungarian empire from the Balkan Peninsula (Martínez-Cruz et al., 2015). This occurred during the Middle Ages, when persecution against the Romanies began. Both the Vlax Roma and the Romungro were subjected to a variety of human rights abuses in an attempt to assimilate them, though all Romani groups in Medieval Europe were subject to mistreatment. For example, the Eastern Europeans tried to take the Vlax Roma’s identities away by enslaving them and separating their children from their families (Martínez-Cruz et al., 2015). By doing this, the children were raised in an environment unlike that of their own people, and were unaware of their original cultures. Also, when they were enslaved, they were forbidden from speaking their mother tongue, leading to loss of the language in later generations. This practice continued in countries throughout Europe until the 20th century (Hajioff & McKee, 2000). Thus, travelling was more than just a way of living; it was a matter of life or death. The westward—and eventual worldwide—expansion of the Romani people dawned when their slavery ended in Walachia and Moldova in the nineteenth century, though more recent movement took place due to other large shifts in the European social environment, such as the Holocaust (Martínez-Cruz et al., 2015). The Holocaust was a significant determinant of Romani migration, especially to the Americas, in the twentieth century. While laws discriminating against the Roma had already been in place for centuries prior to World War II, when Adolf Hitler came to power, new laws were implemented to “cleanse” the Roma from society (Lutz, 1995). During WWII, Romanies were referred to as Zigeunerplague, which comes in part from tsigan for “slave,” and is derived from a Greek word for “untouchable;” it translates to “gypsy plague” (Gheorghe, 1991). And while they were persecuted and exterminated in large numbers in internment camps much like Jewish people, the disabled, and members of the LGBT community, prejudice against Romanies was handled differently in the post-war years. For example, while the German Parliament admitted that the persecution of the Jewish people was based on racial/ethnic grounds, as well as other forms of bigotry for other minority groups, this did not hold true for Romanies. The popular opinion, and the one used to justify continued Romani persecution and deportation from Europe, was that Romanies were slaughtered for social reasons—because they are thieves, criminals, inherently bad people—rather than due to their race, which was the true reason for their mistreatment (Gheorghe, 1991). This was also the reason other ethnic groups were paid financial reparations for the horrors they suffered at the hands of the Nazis, while Romanies were given nothing. This doomed any survivors to generations of poverty, fear of their governments, and mistrust of the people around them. Romanies are an often forgotten persecuted group from the Holocaust; sadly, not only did the Nazis murder a large number of Romanies (over half a million recorded); it also set the ethnic group back several steps in socioeconomic equality, especially after centuries of enslavement and ethnic cleansing (Hajioff & McKee, 2000). The relative recency of the Holocaust is a major reason Romanies are still treated as second-class citizens throughout the continent; however, this does not stop them from finding ways to survive. At a population of between 12 and 15 million people, today, the Romanies constitute Europe’s largest ethnic minority (Martínez-Cruz et al., 2015). They exist throughout the continent and travel the countryside, making trade and doing small work in cities to support their families. While it is largely accepted that Nazi Germany’s treatment of other minority groups was evil, some still believe that the Romanies deserved their fate because they are thieves; a lesser people, a burden to society. Because of this stigma, they continue to face persecution. Generally, discrimination is much more openly practiced—and sometimes violent—in Eastern Europe than Western Europe. A gross example of this is the mass sterilization of Romani women in Czechoslovakia (today the Czech Republic and Slovakia); this occurred between the years 1971 and 1991 (Stoyanova, 2013). They were sterilized both surgically and chemically, often without their knowledge. Jirina Dzurkova, a victim of sterilization, recounts how when she went to the hospital for treatment of an ectopic pregnancy, the staff insisted on an immediate operation; “they didn’t make [her] sign a paper, [and] there was no talk of sterilization at all” (Van der Zee, 2016). The first Romani woman to sue the Czech Health Authority in 2005 was Elena Ferencikova, who suffered from sterilization at the age of nineteen. The court failed to grant her financial compensation, but the hospital apologized for performing the operation without her informed consent (Stoyanova, 2013). No amount of money or written word can ever restore the dignity stripped from a victim of forced sterilization, though, especially when she belongs to a culture that prizes large families. The sad reality is that most people do not know that this infringement of human rights has occurred, despite the atrocity’s recency. The construction of the Czech Republic’s Lety pig farm—a pig farm built on top of the site of a Romani concentration camp called the Lety concentration camp—is proof of the current mistreatment of Romanies that plagues Eastern Europe. While the pig farm was built in the 1970s, it was not until January 2018 that the Czech Republic finally agreed to remove the pig farm, where 327 Romani Holocaust victims—241 of whom were children—died (Gross, 2018). The farm ceased its operations in February of this year (Gross, 2018). But as one can imagine, the remaining tension has yet to dissipate. Romani distrust of the healthcare systems remains, scaring them from seeking sometimes much-needed medical care. Romani-AmericansAn estimated one million Romanies currently reside in the United States; among them are descendants of the Hungarian, Austrian, Russian, and Serbian Roma, the Romnichels, the Ludar, and the Black Dutch, all of whom arrived between the years 1850 and 1914 (Vivian & Dundes, 2004). While this wave of immigrants was large and came with other Europeans, there is evidence that the Roma occupied North America even before then. Christopher Columbus brought the first few Romani slaves (Hancock, 2010). Many of the first Romanies brought to the Americas were also convicts and servants (Ostendorf, 2013). A larger wave of Romani immigration occurred during the 1840s, and another in the early 20th century; recently, since the 1970s, more came to the United States from Eastern Europe (Ostendorf, 2013). This is likely due to the region’s Cold War-related political and economic pressures under the Soviet Union’s communist control. While there are estimated to be at least one million Romanies living in the United States, the U.S. Census Bureau’s 2011-2015 American Community Survey 5-Year Estimates only count 19,164 +/- 1,533 individuals living in the country. This large disparity between the population estimate and the headcount is partially attributable to the Romani travelling lifestyle. In the United States, Romanies can be found living in areas with various levels of population density; how they choose to live their daily lives depends on how the area, whether urban, rural, or somewhere in between, meshes with the ethnic group’s penchant for travel and trade. Romanies who live in rural areas often travel in trailers, campers, or other mobile homes, and may temporarily settle in RV parks (Courbet et al., 1996). Those who live in cities tend to live in poorer neighborhoods, close to main streets; while the homes themselves may be on the smaller side, families are large and come-and-go (Sutherland, 1992). American cities with a significant population of Romani people include New York City, Houston, Los Angeles, Dallas, and others (Vivian & Dundes, 2004). Thus, Romanies tend to live in areas that are considered to be types of food deserts; rural areas are not in close proximity to grocery stores with a wide variety of fresh produce. Meanwhile, inner-city regions tend to have little more besides fast-food restaurants and convenience stores, both of which are low-cost sources of food, but also not the most nutritious options. Geography is just one of the many factors that create challenges to healthy living for Romani-Americans. Another issue that contributes to them not living healthily in America is the fear of seeing a healthcare provider. Romani-Americans are instructed from an early age to lie about their ethnic backgrounds for fear of persecution; for the most part, this has helped them avoid bullying to the violent extremes that are so commonly seen in Europe (Strochlic, 2013). This hiding would certainly explain why the U.S. Census Bureau headcount is so different from the actual population estimate. There has been a bad track record on the part of healthcare systems in mistreating Romanies—at the instruction of the government, too, as was observed with the Czech Republic’s sterilization of women. The lack of trust between Romanies and both the government and healthcare providers not only makes them inclined to hide their identities, but also prevents some of them from seeking help. Romani Culture and HealthRomanies have a complex, old, and rich culture, and it is important for Americans—especially medical service providers—to understand its workings to at least a basic level so that a patient’s desire to adhere to their culture is not mistaken for a lack of compliance. Religion, Morality, and Core ValuesWhile the Roma have distinctive views on life, gender roles, and the afterlife, there is no single official religion. Historically, the ethnicity’s travelling nature led them to adopt the religion of whatever resident country they were occupying, whether to hide their heritage and avoid persecution, or because they were forced to do so through assimilation (Vivian & Dundes, 2004). Some of the distinct superstitious beliefs that Romanies hold in spite of these religious beliefs—which could be Catholicism, Islam, Hinduism, and others—include belief in the conflict between Del (God) vs. Beng (Satan), the importance of charms, and spirits (Vivian & Dundes, 2004). Terms like Zigeunerplague (“gypsy plague”) are ironic because purity and cleanliness are incredibly important to Romani culture, so much so that they view gadje (non-Romanies) as polluted, or marime, because of their lack of attention to specific standards of cleanliness. The most important tenet of purity to Romanies is to keep the upper and lower halves of the body—divided at the navel—separate, as the lower half of the body is marime and considered a source of shame. This separation means that the two halves of the body should not touch in any way, whether it is through direct or indirect contact. It is believed that this idea of purity vs. pollution is a vestige of their North Indian origins, as it relates to ideals of the caste system; also, men are thought to inherently be “cleaner” than women (Vivian & Dundes, 2004). Michael Stewart conducted an ethnographic study in the 1980s for which he stayed with Hungarian Romanies in Harangos; he tells how one Romani woman gasped and snatched a water jug from his hand when he almost used it to fix a washing machine, for if the water from the jug had later touched one’s lips, they were contaminated. This is because washing machine water touches clothes that touch the lower half of the body, which would then touch the mouth if the same water jug is later used for drinking. Romanies will keep two separate sets of containers for these purposes, and will actually often have separate eating utensils and dishware for gadje guests because of the fear of the lower body contaminating the upper. Stewart also discusses how Romanies will clean houses previously inhabited by gadje by bleaching them from the top down; some actually will refuse to enter gadje houses. Romanies care so much about purity and cleanliness that they actually will attribute bad luck and illnesses to a failure to stay clean (Stewart, 1997). One sign of a “polluted” object or person is odor, or khan; while the sight of the lower half of the body is considered shameful, khan is worse because smells enter your nose and mouth as you inhale them, polluting you in the same way as though you are touching the object or person. Such standards of purity make it difficult for Romanies to eat hospital food, wear one-piece hospital garments, and sit for physical exams where a doctor might use the same set of nitrile gloves to examine one’s legs and face. Using public bathrooms, let alone those in a hospital setting that is teeming with illness, could be a particularly revolting experience for the Romani patient. Thus, understanding marime is key to working with Romani inpatients’ behavior, ensuring the highest quality experience possible. Romani people prize the large, multifamily unit; as mentioned below, multigenerational families will often live together under a single roof, with members moving in and out depending on their individual situations. This points to the communal nature of Romani culture—unfortunately, though, this can create tension when hospitalization becomes necessary. Romani culture is largely paternalistic, and this holds applications in the healthcare setting. For example, when a Romani woman is hospitalized, decisions regarding the course of her treatment will most likely be determined by her husband’s parents (Thomas, 1985). One of the four key tenets of medical ethics is the principle of respect for the patient’s autonomy, so this paternalistic cultural value can clash with healthcare professionals’ training. This creates a conflict: should healthcare providers stress personal autonomy regardless of whether this is congruent with the values of a family-oriented culture? Or is it possible—and ethical—to show cultural relativism? What is better for a Romani patient, whose very identity centers on the principle of community: individual health, or dignity? This challenge is actually quite common to healthcare professionals because paternalism and communal decision-making are widely-held cultural practices. It is important to understand whether the patient is competent enough to know what is happening, and let him or her decide whether she wants to know what is wrong; whether she understands her condition, and whether she wants her family to decide. It is also important to try and educate the family about the medical condition, the possible treatment options, and the consequences of each option. This way, we can find a middle-ground and respect both the culture’s values as well as the patient’s health. This underscores the importance of transparency. Keeping all parties involved and as informed as possible could save medical professionals from a host of ethics-related conflicts. More on this topic will be discussed in the American Healthcare section, below. The treatment of disease and matters related to death and mourning are important to the Romanies; thus, it is important for all friends and family to gather in the case of any family emergency that may lead to death. Roma will call their loved ones together, meeting at established locations called vurma to find each other so that they can gather at the side of the ailing loved one (Courbet et al., 1996). When one dies, it is common for the grieving process to be intense, if not quite violent. In hospitals, healthcare workers will be alarmed to see Romani family members cry, scream, pull out their hair, and collapse to the ground in the event of a death (Thomas, 1985). They are very close to one another, so it is especially painful. The Romani funeral will be quite ostentatious, with a large number of family members in attendance. They will try to uphold the belief in good luck, dressing in reds and whites (lucky colors), and tossing coins and other tokens into the grave, so that the departed can have them in the afterlife (Courbet et al., 1996). Because the deceased are associated with bad luck, though, the family will not mention them after the funeral (Sutherland, 1992). Family and RelationshipsRomanies typically live in large, multifamily units. They will travel together in bands—kumpanias—with anywhere from ten to hundreds of extended families (Bradford, 2017). Not all Romanies are mobile, though most are; some choose to live lives just as sedentary as the average American (Ostendorf, 2013). In the kumpanias, elders are responsible for organizing rules, distributing punishment, and making judgments (Bradford, 2017). Principles of inclusion and exclusion are central to Romani culture. Bradford discusses how honor and reputation define a Roma’s place in society, and expulsion from the community is considered to be the most severe form of punishment. While Romanies make for a diverse community, with a variety of different internal laws, they have a strong sense of culture—when gauging whether a person is “one of them,” Romanies will ask not who one is, but who his ancestors are and where he comes from. The principle of familismis pervasive in cultures emphasizing the group over the self, in contrast to the more individualistic Western ideals so prevalent among Americans. Like in other community-based, familistic cultures, family comes first to the Romanies; thus, family ties are highly valued. As Bradford mentions, because they have never had one single country or kingdom, the basic unit of Romani community is the family. Romanies marry young, and are encouraged to have large families. In Bulgaria, almost half of the pregnancies with mothers aged 13-16 were of Romani descent (Hajioff & McKee, 2000). Also, a study in Spain found that Romani women are less likely to use barrier forms of contraception; another study in Bulgaria found that only 61% of Romani women use contraception, and 33% of Romani women have had more than three abortions (Hajioff & McKee, 2000). This can likely also be attributed, at least in part, to their fear of seeking reproductive healthcare on account of Europe’s history of chemically sterilizing Romani women. Due to a lack of available research, though, it is unclear how true this is in the United States. While purity standards are paramount in importance to Romanies, they are even more stringent against women, who cannot so much as be seen going towards the bathroom by a man; as one can imagine, they must also be discreet about their sexuality, with some groups requiring hiding of the hair so as to not appear sexually desirable (Stewart, 1997). Also, to some Romani subcultures, even pregnancy can be a source of shame; it shows that the woman was sexually active, so it must be concealed. The vagina is considered to be a source of pollution due to menstruation; thus, a woman must walk around a man to avoid brushing her skirt up against him and “infecting” him (Courbet et al., 1996). This leads to a number of challenges in the healthcare setting, which will be discussed below. Romani weddings are large and elaborate, as is consistent with Romani appreciation for ostentatiousness (Bradford, 2017). Romanies are encouraged not to marry outside of the group. This leads to consanguinity—otherwise known as blood relations—in marriages. A Spanish study showed that Romanies have nearly twelve times higher rates of consanguinity as the rest of the Spanish population, making recessive congenital diseases seven times more common in the group (Hajioff & McKee, 2000). A study of disease and lifestyle in 58 Romanies in Boston, Massachusetts, yielded that thirteen out of the twenty-one marriages in the sample were consanguineous, making for an inbreeding coefficient of .017 (Thomas et al., 1987). Since their immigration to the United States, Romanies have pursued careers that allow them to align with their mobile nature. They have been animal trainers, census takers, coppersmiths, mechanics, and fortune tellers; accordingly, license requirements and restrictions against fortune-telling have been passed in the United States in efforts to target them (Ostendorf, 2013). Their largely blue-collar work environments create environmental health issues; for example, because of their labor, Romani children are more likely to suffer from burns and lead poisoning than most children (Hajioff & McKee, 2000). Diet and LifestyleThe diet of the average Romani-American is certainly not conducive to their health. The palate calls for fried, greasy foods; a diet heavy in land meats and carbohydrates, and scant in green vegetables. Some tribes believe that feeding green vegetables to a pregnant woman puts her at risk of health problems, and makes the baby more likely to colic (Sutherland, 1992). It is widely known that such an unbalanced diet increases one’s risk of cardiovascular disease, diabetes, hypertension, and certain cancers—and as one would imagine, such a diet so early on in one’s life could have profoundly negative consequences for child development. On a similar note, it is well known that in some cultures, higher weight—especially in men—is a symbol of prosperity, as he has access to great amounts of food. Romanies are no exception. The Roma believe that such prosperity as expressed by overweight is indicative of good luck, which is critical in significance to Romani culture (Vivian & Dundes, 2004). These lifestyle choices can lead to poor health outcomes, unsurprisingly. In the sample of 58 Roma from Boston, Massachusetts mentioned above, 46% had diabetes, 57% had hypercholesterolemia, 73% had hypertension, and 80% had hypertriglyceridemia; among these people, 86% smoked cigarettes and 84% were obese (Thomas et al., 1987). Disproportionate poverty risk, difficulty of access to nutritious foods (due to the areas they inhabit often being food deserts), and lack of education regarding the importance of a healthy diet only serve to worsen the issue. With so many factors influencing the Romani palate—as well as genetic precursors to obesity, which will be discussed below—it is easy to see why they are more likely to suffer from obesity-related health consequences such as cancer than the average American. Because this condition is heavily reinforced by cultural beliefs, though, gadje (especially in healthcare) must be mindful when approaching the topic to avoid causing offense. EducationRomanies fear that extensive intermingling with gadje will corrupt their children; for this reason, young Romanies who are sent to American public schools may be withdrawn between eight and eleven years of age, and taught the ways of adult Romani life (Bodner & Leininger, 1992). They speak Romane, an unwritten tongue based on the ancient language of Sanskrit (Bodner & Leininger, 1992). Moreover, they do not keep written history of births, deaths, or census, so it is difficult for gadje to keep track of them (as is clear by the aforementioned disparity between the U.S. Census headcount of Romanies and the estimated Romani-American population). This speaks to the exclusive, insular nature of Romani culture. While American educators have made attempts to integrate Romani-Americans into the American public school system, these efforts have been limited and largely unsuccessful. For example, California’s Children’s Hospital in San Francisco attempted to establish an alternative schooling program for Romanies in 1965 (Courbet et al., 1996). Due to a multitude of factors, from insufficient funding to difficulties in establishing a strong faculty base, this was unsuccessful. A silver lining to the lack of knowledge of American Romanies has been the lack of protest against their presence in schools—partially because there are not many in schools in the first place, and also because the children are taught to hide their identities from their classmates. In contrast, they are not received well in Europe, where people know who the Romanies are. A few horror stories include Romani schoolchildren in Zaragoza, Spain, being pelted with bricks in 1984; also, in Italy, car tires were piled onto roads and set ablaze to prevent Romani children from making it to school (Courbet et al., 1996). Meanwhile, in Hungary, in the 1980s, an estimated 15% of Romani children were placed into schools for mentally-handicapped children (Courbet et al., 1996). This attitude has not gone away. In 2017, Ben Bennett, a 13 year-old Romani boy from England whose dream is to be either a pilot or the Prime Minister, was forced out of eleven different public schools; he claims that it is the teachers who are more prejudiced than the pupils (Brennan, 2017). After being excluded from his class at age ten, Bennett says, “'when I asked why it was, [the teacher] said because I am a gypsy other pupils don't feel comfortable around me and she doesn't feel comfortable teaching me’” (Brennan, 2017). His mother finally withdrew him from public school in May 2017 after Bennett and his sister were attacked by sixteen boys. This also exists in the United States, though less so because—as mentioned before—Romanies hide their identities. 34-year old University of Alaska grant writer Kristin Raeesi, a Romani-American activist, recounts some of the discrimination she faced as a child in her interview with Daily Beast contributor Nina Strochlic. Raeesi describes the discomfort she felt as a young child when, during an elementary class, she sat through a reading of renowned American poet Shel Silverstein’s poem, “The Gypsies are Coming” (Figure 1); after that day, she chose not to tell her classmates about her Romani identity (Strochlic, 2013). “The Gypsies are Coming” was published in the 1974 edition of Where the Sidewalk Ends: the Poems & Drawings of Shel Silverstein (Hoefling, 2017).
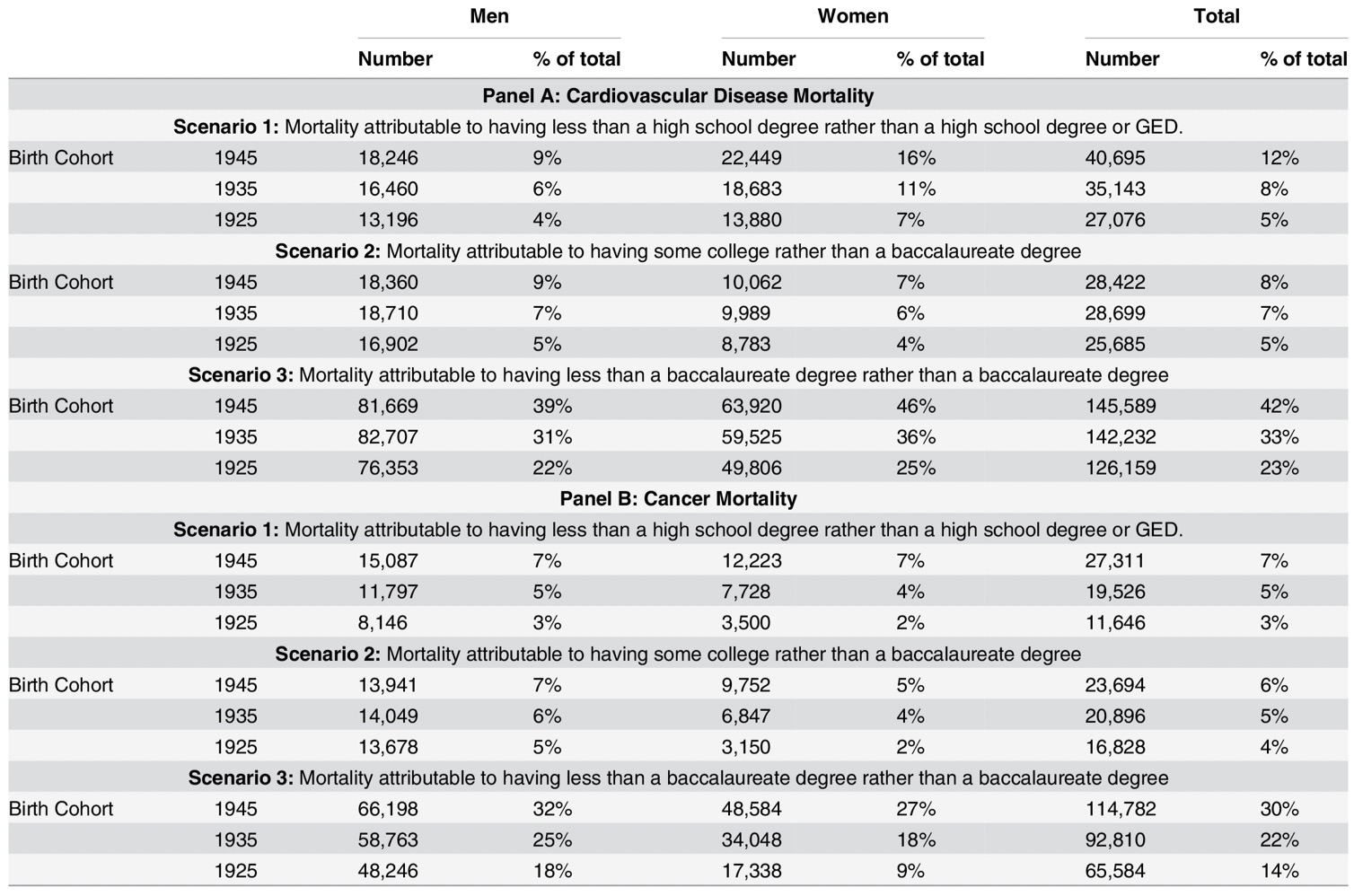
Figure 1. Photographs of pages showing “The Gypsies are Coming” by Shel Silverstein (Hoefling, 2017). Silverstein changed “gypsies” to “googies” in later editions of the book after facing backlash for the poem (Hoefling, 2017). It is difficult to give Silverstein the benefit of the doubt as ignorant of the racially-charged meaning behind these words. The accompanying illustration features a woman with the large nose, dark hair, and elaborate garb associated with antiziganist (anti-Romani) stereotypes. Later, during a Balkan music class at the University of Wyoming, when a guest lecturer said that the Roma were a “dirty and culture-less people,” undergraduate-aged Raeesi tearfully decried the speaker for her racist language (Strochlic, 2013). Her experiences in school, however hurtful, are part of what inspire Raeesi to tirelessly pursue her work in Romani activism today. She now strives to educate the American public about Romanies in any way that she can. Increasing public awareness of the Romanies is important because due to their hiding of their identities, almost any media portrayal of the group—however flawed—sways Americans’ perceptions. For example, Glenda Bailey-Mershon, who tutors Romani-American children in North Carolina, tells of how her students were bullied relentlessly in school after the show “My Big Fat American Gypsy Wedding” first appeared on TLC in 2012 (Strochlic, 2013). This type of bullying can teach children that school is a place for harassment rather than education, and that negative association may be enough to demolish any of their hunger for knowledge entirely. With these instances in mind, it is no wonder that Romanies across the world, including in the United States, fear sending their children to public school. This prevents Romani children from becoming educated and empowered in today’s Western society. Even if a Romani-American child or adult hopes to receive an education, the lack of attention to their cultural values prevents them from succeeding. Unfortunately, a lack of education can potentially have dire health-related consequences, too. According to Dr. Patrick Krueger, an assistant professor at the University of Colorado-Denver’s Anschutz Medical campus, education is the best way to relate socioeconomic status with mortality because it stays constant over the course of one’s life, and can be affected by policy intervention. Krueger et al. conducted a study titled “Mortality Attributable to Low Levels of Education in the United States;” through analysis of data gathered from over one million individuals aged 25 to 85 (from an NHIS survey that took place from 1986 to 2004), it was found that education level was inversely related to mortality rates from cardiovascular disease, cancer, and other causes of death (Krueger et al., 2015). This study asserts that 545,525 deaths per year are indirectly attributable to not attaining at least a baccalaureate degree. There are a variety of ways in which education can affect one’s health. Krueger et al. point out that it enhances cognitive development, encourages compliance with medical treatment, and improves psychological state (Krueger et al., 2015). Education leads to higher levels of social capital, which is defined as social resources and support. It can also help individuals obtain employment in better jobs, which are often less hazardous and pay more generously, allowing for the ability to live in safer neighborhoods, eat better diets, have health insurance, and afford better healthcare. Both lack of social capital and lack of stable career-related resources can lead to increased levels of stress, which is detrimental to health outcomes. Finally, of course, lower levels of educational attainment restrict health literacy because people who lack higher education are less likely to have been taught the importance of diet, exercise, and not smoking. As shown in Table 1, in the 1945 birth cohort, 7% of cancer deaths in both females and males were correlated with not having at least a high school degree.
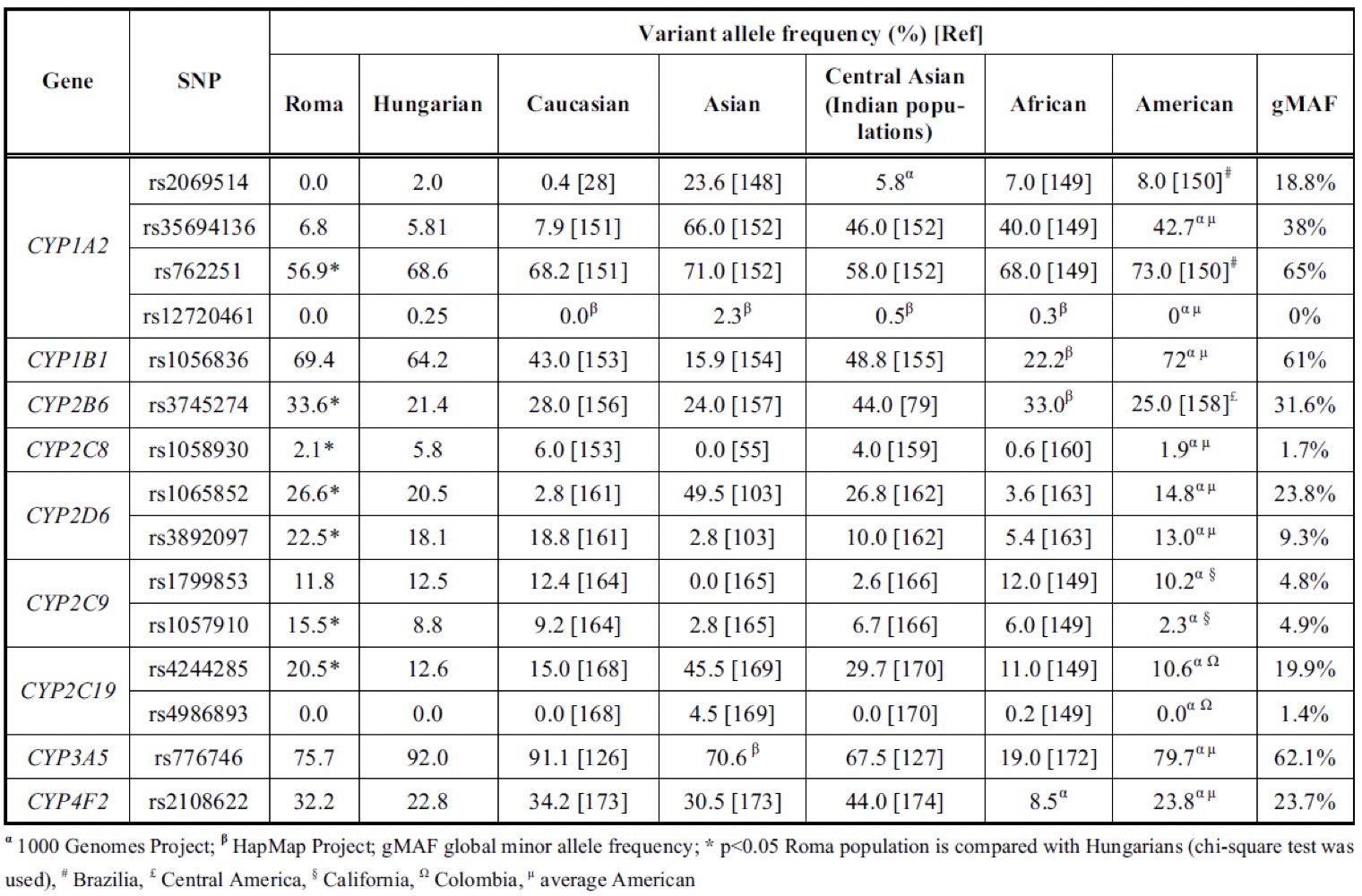
Table 1. Cardiovascular disease and cancer mortality across different educational attainment groups by gender and generational cohort (Krueger et al., 2015). Interestingly, this inverse effect between education level and mortality was shown to be stronger in groups that are less likely to obtain an education in the first place. In other words, those who are born into lower socioeconomic backgrounds, lack parents with high educations, or lack access to institutions of education benefit more in terms of health than those without these disadvantages when offered a higher education (Krueger et al., 2015). This could mean that education would similarly lead to significantly better health outcomes for Romani-Americans, potentially making it an effective target of policy action. Experience with American HealthcareCultural concepts of fortune, family, and purity affect the everyday lives of Romanies, from their interactions among themselves to their interactions with healthcare systems. The behaviors that they exhibit can be confusing or even scary to the medical provider who does not understand the cultural context, and the resulting misunderstandings create barriers to successful care. As such, it is important to remember these cultural elements when treating the Romani-American. The four principles of medical ethics are as follows: respect for patient autonomy, non-maleficence (the principle of “do no harm”), beneficence (aim to do the highest level of good for the patient) and justice (respect for human rights, the law, and fair allocation of resources). In the United States, healthcare professionals strive to adhere to these principles. But when handling patients with distinct, relatively unknown cultures, sometimes cultural values and healthcare ethics can clash. In “The Crossroads of Culture and Health Among the Roma (Gypsies)” Carrie Vivian and Lauren Dundes discuss the reality of racial profiling in the healthcare setting. Romanies face stereotyping that leads to medical staff being reluctant to offer them treatment. For example, if Romanies are viewed as people who are dishonest and who move frequently, they are seen as people who are less likely to pay their bills—in reality, though, Romanies are just as likely to pay their bills as anyone else (Vivian & Dundes, 2004). In fact, not doing so would violate the Romani cultural principle of maintaining good luck by paying all debts (Thomas, 1985). To steal would give him bad luck; as such, it is incredibly unlikely—or at least, no more likely than it would be for another American—that a Romani-American would intentionally make off with loaned money, or not pay their medical bills. This is just one example of the ways that prejudice in healthcare is harmful. Because Romanies want to stay close to their families, and will feel anxious and threatened if isolated, they will accompany family members to hospitals—not just in small numbers, but sometimes with entire families camping around the hospital (Sutherland, 1992). This is problematic for healthcare workers because they do not understand how to handle this aspect of the culture in a sensitive way such that they can do their duties as healthcare professionals. A way to mediate this situation is to respect this tenet as much as ethical standards within the hospital permit, and allow the families to accompany their loved ones into the exam room. While this holds true for all situations, it is especially important in the context of death. Romanies believe that during anesthesia, the patient is undergoing a “little death” because they are put under an almost comatose state of unconsciousness (Vivian & Dundes, 2004). Because of this, they avoid any medical procedure requiring total anesthesia whenever possible. This fear can lead Romanies to avoid life-saving surgical procedures, such as the removal of a potentially malignant growth to prevent metastasis. As mentioned earlier, Romanies like to be with their family members during death. Because total anesthesia is regarded as “little death,” it follows that Romani family will desire to surround a loved one who agrees to undergo a surgery during their time in the recovery room (Vivian & Dundes, 2004). This has the potential of aggravating healthcare providers who do not understand the culture, putting the two at odds with each other, and creating a negative experience that may prevent that particular family from wanting to see a healthcare provider again in the future. A lack of understanding of the suggested medical procedure, and not knowing what is taking place in the other room, could worsen any anxiety felt by the family members during their loved one’s time in surgery. Transparency is key to alleviating fears, and full disclosure of any relevant medical procedures to the patient and their family (if the patient desires, though this will likely be the case with Romanies) not only helps accomplish this, but is the most ethical course of action healthcare providers can take. Romanies will usually not see a healthcare provider until it is absolutely necessary, which is a high-risk behavior and potentially dangerous to one’s health (Sutherland, 1992). For minor ailments, such as the common cold, indigestion, mild skin conditions, and the like, they will self-medicate with homeopathic remedies such as herbal poultices. Sometimes they will do so even for more severe conditions. For example, one woman was documented to have treated her breast cancer with garlic presses (Thomas, 1985). There are a variety of reasons for this, such as the cost of modern western medicine, the cultural significance of herbal remedies, and ease of access to herbs, to name a few. But one of the most likely reasons for their reluctance to see healthcare professionals is distrust. As discussed above, Romanies have quite recently suffered from human rights violations ranging from forced sterilizations to genocide. If it is truly necessary to see a healthcare professional for a certain ailment, though, Romanies not only will go to a doctor—they will seek out the best healthcare that they can buy, pursuing care from what they will call the “biggest” doctors (Thomas, 1985). These doctors are the ones with the most prestigious professional degrees, the best reputations, and/or the highest treatment success rates. While social predispositions to disease make for important talking points in any study examining cancer epidemiology in an ethnic group, it is also critical to examine biological risk factors for the disease. The second half of this thesis examines a number of key precancerous risks at the molecular level. Some of these are genes encoding cell membrane surface receptors, transmembrane proteins, and cytokines. Most have functions relating in some way to cellular metabolism. Biological Risk Factors for CancerGenetic Predispositions to Cancer and Relevant BiomarkersIt is important to note that most of the studies discussed in this section were not conducted in the United States; rather, they were conducted in Eastern Europe, where a majority of today’s Romanies live. While the geographical, political, and demographic climates are different between the two regions, I believe that the high degree of insularity of Romani culture keeps certain (often severe) genetic complications within the group. Also, the biggest wave of Romani immigration to the U.S. occurred in the early to mid- 20th century, which was only a few generations ago. Thus, the Romanies sampled in these studies are genetically similar enough to Romani-Americans to make the results worth consideration in this context. At the same time, I want to reiterate that the dearth of research in Romani-American genetics is one of the many reasons I am writing this thesis. There is clearly a gaping hole in this field; I hope this discussion will bring it to the attention of American molecular geneticists and epidemiologists and inspire them to pursue research on Romani-Americans. With the host of political changes and wars that have recently taken place in Eastern Europe, such as in former Yugoslavia, Romanies have exhibited increased east-west migration patterns (Kalaydijeva et al., 2001). The genetic climate of European Romanies, and possibly American Romanies, has been changing accordingly. Cytochrome P450 Gene FamilyIn humans, cytochrome P450 enzymes (CYPs) are expressed primarily in liver cells (hepatocytes), and are responsible for metabolizing potential toxins. CYP is subdivided into 18 families, containing approximately 60 distinct genes; these genes together account for around 70-80% of enzymes involved in drug metabolism, making them highly effective targets for chemotherapeutics (National Institute of Health, n.d.). In this thesis, CYP families 1, 2, and 3 will be investigated because families 1 through 3 account for between 70-80% of phase 1 metabolism of clinically significant drugs. However, additional research is necessary to determine how the other CYP families affect Romanies. In their 2016 literature review, Szalai et al. examine CYP genotype frequencies and find a number of variants that are clinically significant in Romanies. CYP1A2 is a member of the first family in the cytochrome P450 gene group; polymorphisms are slight differences in the nucleotide sequence of a gene, which can affect the function of the expressed protein in minor or major ways. Szalai et al. hope to compare the effects of these mutations in Hungarians and Romanies. It was found that different polymorphisms have different effects in the subgroups—for example, increased CYP1A2 induction resulting from tobacco use is more likely to cause cancer in Romanies with the -2467delT polymorphism. Of particular interest is the way that tobacco use, especially smoking, interacts with these polymorphisms to increase cancer risk in both populations. Not only does this show that Romanies are more likely to have certain mutations that increase cancer risk; it also shows that Romanies have genetic predispositions to cancer that are exacerbated by the unhealthy lifestyle choices (such as tobacco use) so prevalent in the ethnic group. CYP1B1 is critical in preventing cancer, and will be discussed in greater detail below. It is most well-known as a causative determinant of primary congenital glaucoma (PCG), an autosomally recessive disorder with a multifactorial genetic phenotype that causes blindness (Szalai et al., 2016). In the Szalai study, though, its significance as a gene conferring susceptibility to cancer is most important. It functions both as an early-stage tumor marker and a hallmark of carcinogenesis, and is expressed in adipose tissue and in the nervous system, uterus, prostate, fallopian tubes, kidneys, lungs, spleen, and eyes. CYP1B1 is important in the taxane, estrogen, and amodiaquine pathways, giving it utmost importance in the metabolism of taxane (paclitaxel and docetaxel) chemotherapeutics, which are anti-mitotic. CYP1B1*3 mutation in particular is associated with lower long-term survival rates in patients offered docetaxel treatments for breast, non-small cell lung, and ovarian cancers. Szalai et al. found that Romanies were significantly more likely to exhibit the *3/*3 genotype (50.1% frequency) of CYP1B1*3, compared to Hungarians (39.3%), Indians, and Caucasians of all countries, leading to lower survival rates in cancer patients treated with docetaxel. It is thus important to study this not only because it predisposes cancer development; it also hinders efforts in anticancer treatments, leading to lower survival. In the second CYP family, the gene CYP2C9 is responsible for the metabolism of up to 15% of drugs, including antidiabetics, antimicrobials, anticoagulants, angiotensin II receptor blockers, and non-steroidal anti-inflammatory drugs (NSAIDs), to name a few (Szalai et al., 2016). There are a variety of different alleles for this gene; one of the first discovered and most-researched is the CYP2C9*3 variant. In people expressing this allele (as well as CYP2C9*2, for that matter), metabolic enzymes resulting from the expression of the gene are lower activity than other polymorphisms—as they are decreased-function alleles—so lower doses are necessary to prevent overdose and serious harm. Szalai et al. found that Romanies are over three times more likely to express the pernicious *2/*3 genotype than Hungarians—at 4.7% compared to 1.5%. Romanies also carry the SNP rs1057910 at a rate of 15.5%, compared to 8.8% in Hungarians and 2.3% in Caucasians. In alignment with these results, compared to both Hungarians and Caucasians, Romanies have significantly lower extensive-metabolizer phenotypes for CYP2C9 and higher intermediate- and poor-metabolizer phenotypes. This means that dosages between these ethnic groups for drugs that target metabolic processes related to this gene should not be treated the same way. Romanies should have lower dosages in order to ensure better health outcomes. Given that common NSAIDs are Aspirin and Ibuprofen, which are widely-used, over-the-counter drugs, it is important for healthcare providers to keep this in mind. Another CYP gene in family 2, CYP2C19, is important in metabolizing drugs responsible for inactivating proton-pumps in the electron transport pathway, metabolizing certain antidepressants, and in activating the anticoagulant agent clopidogrel (Szalai et al., 2016). As with most of the CYP genes, it is expressed in the liver. In their 2013 study of the pernicious and oncogenic CYP2C19*2 allele mutation in both Romani and Hungarian samples, Sipeky et al. analyze differences in the frequency of the mutation between DNA samples from Romanies and Hungarians. There were three genotypes assessed: *1, *2, and *3. Combinations of the alleles and their incidences were studied in different ethnic populations besides just the Roma and Hungarians. Consistent with other research demonstrating Romani origins from modern North India, Sipeky et al. found that Romanies are genetically similar to today’s Northern Indians. Results showed that the Roma are more likely to have pernicious mutations at position 2* of the CYP2C19 gene when compared to the rest of the population (Sipeky et al., 2013). In fact, when compared to other ethnic groups, the intermediate-metabolizer (IM; *1/*2 genotype) and poor-metabolizer (PM; *2/*2) were significantly higher in Romanies than Hungarians and Caucasians, with the IM genotype frequency being 31.8% and the PM frequency being 4.6% (Szalai et al., 2016). Hungarians had IM and PM frequencies of 23.0% and 1.1%, respectively, and Caucasians were found to have 24.7% IM and 3.8% PM frequencies (Szalai et al., 2016). Delving further into the second CYP family, Weber et al. (2015) found that Romanies are more likely to carry phase I Cytochrome P450 enzymes 2B6 and 2D6 mutations than Hungarians. The mutation frequency of CYP2B6 c.516G>T was significant at p < 0.001, as was CYP2D6 c.100C>T at p = 0.003, and c.1846G>A at p = 0.022 (Weber et al., 2015). To understand what this means, one must remember that there are four nucleotide base pairs: adenine (A), thymine (T), cytosine (C), and guanine (G). The notation CYP2B6 c.516G>T means that for enzyme CYP2B6, the allele at locus 516 has a polymorphism—or single nucleotide switch—from G to T. In the study, it was 33.6% in the Romanies, compared to only 21.4% in Hungarians. CYP2D6 100T was 26.6% in Romanies and 20.5% in Hungarians. And the 1864A polymorphism frequency was at 22.5% in Roma and 18.1% in Hungarians. This means that for these four sites, Romanies had higher percentage rates of mutations, leading to a slightly different genetic code for the CYP2D6 gene and differential protein expression—and thus—differential metabolic processes associated with the protein. There was also an increase in homozygous minor allele genotypes in Roma participants compared to Hungarian ones. This pharmacogenetic data has clinical significance because it changes the way that certain chemotherapeutics—primarily those that may target these enzymes—operate in killing malignant cells. In the third CYP family, CYP3A5 is important in the metabolism of anticancer drugs tamoxifen, cyclophosphamide, irinotecan, and gemcitabine (Szalai et al., 2016). It was found that Hungarians express the CYP3A5 variant *3 genotype *3/*3 at a rate of 84.9%, compared to 53.9% in Romanies; Hungarian samples were found to have similar rates to other Europeans and Americans. This means that Romanies will metabolize taxane chemotherapeutics more efficiently than these other ethnic groups. Health outcomes of Romani cancer patients being treated with these drugs should thus be monitored, and dosages adjusted accordingly if the standard causes especially adverse side effects. Clearly, there are a variety of CYP allele variants that not only differ in frequency between Romanies and other populations, but also have important pharmacogenic consequences. An interethnic analysis of some of the mentioned CYP variant frequencies, as well as other CYP variants, is illustrated in Table 2.
Table 2. A comparison of variant allele frequencies in CYP among different ethnic groups. (Szalai et al., 2016). PRDMThe PRDM1 gene is involved in key cellular processes related to development, such as apoptosis (cell death), differentiation (when cells are “assigned” their roles), and proliferation; abnormalities in any of these processes can lead to cancer (Varszegi et al., 2014). A correctly-functioning PRDM1 protein codes for a zinc finger—a type of polypeptide containing a zinc ion—responsible for repressing cellular transcription, which creates messenger RNA (mRNA) using a cell’s DNA, and later down the line, lowering gene expression. When a protein that represses transcription is not expressed correctly, cells transcribe too much mRNA, expressing certain genes more—in the case of PRDM1, lowered expression leads to less apoptosis and more proliferation. The SNPs rs4946728 and rs1040411 cause lower PRDM1 excretion, and are implicated in secondary malignancies in pediatric Hodgkin’s lymphoma patients treated with radiotherapy (Varszegi et al., 2014). In one clinical study, Dr. Dalma Varszegi et al. (2014) sought to determine whether Romanies and Hungarians differ from the average (denoted by three control groups based on individuals self-identifying as non-Hispanic European white people who had also received radiotherapy for Hodgkin’s lymphoma) in terms of rs4946728 and rs1040411 incidence. It was revealed that Hungarians and Romanies did not significantly differ in their allelic profiles for these variants; however, Hungarians and Romanies were more likely to carry the rs4946728 risk C allele compared to both the discovery and combined control variables (79.4% in Hungarians and 83.5% in Romanies vs. 59.1% in Hungarians and 63.7% in Romanies; p < 0.05). The same held true for the homozygous carriers for the rs1040411 risk A allele. Also, heterozygous carriers of this allele were more prevalent in Romanies than all three control groups. This information is important because it could serve as a screening target in Romanies treated for pediatric Hodgkin’s lymphoma. If healthcare providers screen them for these risk alleles, they can be kept under watch for any recurring cancers later on, which would increase the likelihood that the disease can be discovered and treated in time to improve the patient’s odds of a positive outcome. AdiponectinIn 2014, Petrášová et al. conducted a study sampling 452 Romanies from Eastern Slovakia. In that sample, not only were close to a quarter of the participants overweight, but participants also had higher than normal cholesterol, triacylglycerol, and LDL-cholesterol levels—all of which are biomarkers indicative of overweight. On the other hand, their HDL-C and adiponectin (APN) levels were lower compared to the average (Petrášová et al., 2014). Such a difference in APN levels has significant physiological consequences. APN is a hormone secreted by adipocytes (fat cells) that assists in metabolizing glucose and lipids (Hebbard & Ranscht, 2014). In their study of the roles of APN in cancer, Hebbard & Ranscht found that low levels of this biomarker have been linked to malignancy in tumor cells. In cancer patients—especially for obesity-related cancers such as those of the digestive and hematological systems—not only are circulating APN levels low, but these low levels have suggested an inverse relation to malignancy, causing faster progression in cancer patients (VanSaun, 2013). One mechanism through which APN mediates tumorigenicity is through its association with T-cadherin to promote angiogenesis. Angiogenesis in tumors—which is when the tumors attract blood vessels to supply them with oxygen, nutrients, and growth factors—is a distinctive feature of cancer cells; Hebbard & Ranscht found in a clinical study involving model mice that when APN is knocked out in breast cancer patients, the tumors adapt to the hypoxic environment and become metastatic, spreading to the lungs and decreasing survival. Another important mechanism through which APN mediates tumor cell progression is through its interactions with insulin and cell growth factors. Insulin interacts with phosphoinositide 3-kinase (P13K) enzyme to initiate the mammalian target of rapamycin (mTOR) pathway—which is pro-oncogenic because it causes cell growth and cell cycle progression. APN functions as an inhibitor of the P13K/AKT/mTOR pathway because it associates with adaptor protein APPL1 and activates protein kinase AMP-activated protein kinase AMPK (VanSaun, 2013). AMPK phosphorylates regulatory-associated protein of mTOR (RPTOR), preventing it from associating with mTOR complex 1 and inhibiting it; mTOR regulation is important because mTOR is responsible for controlling the cell cycle by regulating transcription of hypoxia-inducible factor 1α (HIF1α) cyclin-D1 and c-myc (Hebbard & Ranscht, 2014). Figure 2 provides a visual representation of the P13K/AKT/mTOR pathway. Overactivity of this mTOR signaling cascade—which is caused by an environment of dense nutrients—is problematic because it causes excess cell proliferation, leading to cancer. Therefore, if Romanies have low levels of adiponectin, they are less likely to inhibit mTOR, and their cancer cells are more likely to be metastatic—and thus, deadly.
Figure 2. A diagram of the mTOR pathway. APN phosphorylates and activates AMPK (turning it to pAMPK), inhibiting the mTOR pathway (VanSaun, 2013). LAMB3 splice-site mutationsEpidermolysis bullosa is a severe skin disorder with an autosomal-recessive pattern of inheritance; it leads to death, usually within a few months of the affected patient’s birth (Mayer et al., 2016). After several Romani children in a region of Hungary were born with lethal Herlitz-type junctional epidermolysis bullosa, Mayer et al. sought to determine the reason. Single-nucleotide polymorphisms in LAMB3 compromising laminin-332 were the culprit, specifically the intronic splice-site mutation 1133-22G>A (Mayer et al., 2016). Laminin-332 is a glycoprotein which essentially holds the skin together. Thus, if it is not functioning correctly, the skin can blister or break. In the Mayer et al. study, 306 Hungarian Roma were screened for splice-site mutations in LAMB3; interestingly, out of the 64 Roma who volunteered for screening from one closed community, 30 carried the mutation, whereas none of the other Roma throughout the country did (Mayer et al., 2016). This pointed to the possibility of a founder effect at play, since only that closed community exhibited this particular mutation at such a high frequency. The commonality of founder effects in isolated ethnic groups such as Romanies makes it difficult to generalize them, which is why it is of utmost importance to gather a variety of samples from Romanies throughout different regions and screen for cancer-causing or other debilitating mutations. While mutations in LAMB3 might be common in some parts of Europe, it is uncertain how common it would be here in the United States. More research needs to be conducted regarding the incidence of this mutation in the United States so that Romani-Americans can be made aware of the mutation and know of the possibility of it appearing in children. We must watch for incidences of this rare disease and study any patterns in Roma communities in the United States of epidermolysis bullosa or cancers related to laminin-332. According to The Human Protein Atlas, a resource commonly used to determine oncogenicity of different protein mutations, LAMB3—which is responsible for providing the blueprint to laminin-332 production—is also an unfavorable marker in renal, lung, and pancreatic cancers (The Human Protein Atlas, n.d.). In their study to determine the relationship between laminin-332 expression and carcinogenesis, Tsuruta et al. found that expression of laminin-332 is downregulated (suppressed) in colorectal carcinoma, prostate cancer, breast cancer, and oral small-cell carcinoma (Tsuruta et al., 2008). Meanwhile, it is upregulated and associated with higher tumor invasiveness in cervical cancer, pancreatic cancer, urinary bladder urothelial cancer, gastric cancer, colorectal adenoma, and others (Tsuruta et al., 2008). Thus, if Romanies are more likely to carry mutations in LAMB3 that affect how the critical structural protein laminin-332 appears in the skin, it is possible that they are at risk for associated cancers. Further research is necessary to reveal the incidence of such malignancies in Romanies, as well as the degree of causation between LAMB3 mutations and the mentioned cancers. SLCO1 splice-site variantsSLCO1B3 transporter (Solute Carrier Organic Anion Transporter Family Member 1B3) is a transmembrane receptor in the liver—though also found in the placenta and tumor cells—that is responsible for moving anions across the cell membrane (Nagy et al., 2015). Any mutations in SLCO proteins can affect drug metabolism because drugs and metabolites may struggle to cross the hepatic cell membrane, lowering the efficacy of chemotherapeutics and other drugs. Such mutations conferring an overexpression of genes that facilitate metabolism can also lead to oncogenesis. The membrane protein SLCO1B3 is necessary in the metabolism of taxane anticancer drugs, such as paclitaxel and docetaxel, as well as the immunosuppressant methotrexate. Dr. Agnes Nagy et al. (2015) found statistically significant differences in the incidences of both the 334T>G polymorphism and 1683-5676A>G allele variant in the Roma population compared to the Hungarian one. It was found that SLCO1B3 c.334T>G was significantly different between Romanies and Hungarians, with frequencies 41.54% and 8.04% for the 334 GG homozygous genotype, respectively. Meanwhile, in the 1683-5676A>G variant, the GG genotype was found to be 2.01% in Hungarians and .43% in Romanies. This study also compares the allele frequencies of SLCO1B3 c.1683-5676A>G and c.334T>G in Romanies and Hungarians to those in people of different ethnic groups. Out of all the ethnic groups surveyed—including Caucasians, Indians, Africans, and Chinese—Romanies had the lowest SLCO1B3 1683-5676G frequency. The difference is drastic; the allele frequency rate is 3.4% in Romanies, 15.1% in Hungarians, and 14.7% in Caucasians. And regarding the 334T>G polymorphism, both Romanies and Hungarians had a markedly lower polymorphism rate than the Caucasians. While the authors concede that the study was unable to functionally characterize the pharmacokinetic effects of these genetic disparities, they posit a reason behind the markedly increased risk of conditions such as leukopenia for Hungarians compared to Romanies upon treatment with certain drugs. Thus, while we do not know exactly what the consequences of these polymorphism rates are, it is likely that they contribute to interethnic differences in taxane and other chemotherapeutic drug metabolism ability. It also affects how Romanies respond to certain dosages of chemotherapeutics. For that reason, to ensure the best possible chances of survivorship, interethnic differences in relevant genes must be taken into account when treating Romanies with cancer. In another 2015 study by Nagy et al., variations in SLCO1B1 haplotypes and their consequences were examined between Romanies and Hungarians. SLCO1B1 is a member of the Solute Carrier Organic Anion Transporter family, and is normally expressed in the liver. 470 Romanies and 442 Hungarians were genotyped for variations in c.338A>G, c.521T>C, and c.1498-1331T>C mutations. It was found that Romanies show higher rates of mutation in all of these groups except for c.1498-1331T>C. This has direct implications in statin therapy (cholesterol reduction) because it affects substrate (LDL) uptake into liver cells. It could also potentially affect chemotherapeutic agent penetration (Nagy et al., 2015). The liver is a remarkably fast-growing organ—in fact, it is the only internal organ that is known to have the capacity to regenerate. Therefore, it is a common site for oncogenesis. If Romanies are disproportionately likely to express defective, precancerous gene mutations in liver cells, they are more likely to suffer from liver cancer. ABCG2 and breast cancerA mutation in ABCG2, otherwise known as the breast cancer resistance protein, leads to resistance against a variety of chemotherapeutics (Saison et al., 2012). Such a mutation would make the treatment of breast cancer much more difficult. ABCG2 is critical to the molecular makeup of a type of blood group antigen system called Junior (Jr). In other words, a mutation in ABCG2 affects the way blood cells present Jr, which is likely the reason chemotherapeutics would fail to work properly. The Jr(a-) blood type is uncommon overall, but a significant number of cases have been found in European Romanies. Saison et al. (2012) found that a high Jr(a-) blood type is related to mutations in ABCG2. This indicates that Romanies in Europe are more likely to display the Jr(a-) mutation; thus, they are more likely to have the breast cancers associated with the mutation. Lynch SyndromeHereditary nonpolyposis colorectal cancer (HNPCC) is today considered to be a misnomer. While the name implies that the disease involves only hereditary colorectal cancers (CRCs), over time, it was discovered that the syndrome increases the odds of developing cancers of the stomach, brain, ovaries, hepatobiliary tract, and uroepithelium (de la Chapelle, 2004). Thus, it is now called Lynch Syndrome to encompass those other forms of cancer. Lynch Syndrome is caused by germ-line (heritable) mutations in mismatch repair (MMR) genes PMS2, MLH1, MSH2, and MSH6; penetrance (how often it is expressed and appears when the individual has the genes for it) rates are 80% in colorectal cancer, making that the highest, 60% for endometrial cancer, and 20% or below for other forms of cancer (de la Chapelle, 2004). Not all colorectal cancers are caused by Lynch Syndrome, however. It is estimated that approximately 5% have any association with the syndrome (de la Chapelle, 2004). This number is not concrete. As previously mentioned, there are a few different MMR genes, and the statistics associated with incidence depend on which genes one might use to define Lynch Syndrome. For example, when Lynch Syndrome is operationally defined to include cancers occurring due to mutations in MMR genes, studies have shown association frequencies ranging anywhere from less than 1% to 2.5% (de la Chapelle, 2004). Regarding the other forms of cancer, their association with Lynch Syndrome is uncertain. One form of Lynch Syndrome is known as Muir-Torre Syndrome. Muir-Torre Syndrome victims are at risk of developing the colorectal, endometrial, gastrointestinal, and hepatobiliary cancers brought by Lynch Syndrome; they are also at risk of developing cancers in their sebaceous glands (Muir-Torre Syndrome, 2014). Sebaceous glands are located in the skin, and are so named because they are responsible for the secretion of sebum (oils). A patient with Muir-Torre Syndrome will exhibit sebaceous adenomas, epitheliomas, carcinomas, and kareatocanthomas, which are mostly noncancerous lumps or cysts, save for the carcinomas (Muir-Torre Syndrome, 2014). The mismatch repair genes most commonly associated with Muir-Torre Syndrome were MLH1 and MSH2, and Muir-Torre Syndrome is autosomally dominantly inherited, meaning that an individual need only have a single copy of the gene to develop the disease (Muir-Torre Syndrome, 2014). Dr. Henry Lynch, the namesake of Lynch Syndrome, conducted a case study in 1998 of the incidence of CRC and Muir-Torre Syndrome in a Romani family. In that family, it was found that hMSH2 germ-line mutation was present, and that it served as a reliable predictor of the development of Muir-Torre Syndrome (Lynch, 1999). This shows that Lynch Syndrome is present in Romanies; even though this was a case study of a single family, because Lynch Syndrome is expressed as an autosomal dominant condition, it is possible that more Romani families across the world carry the genes for the condition. This is especially true given the high degree of consanguinity in Romani culture. Of course, though, it is difficult to tell to what level CRCs in Romanies are attributable to genetics alone when the unhealthy lifestyle choices so prevalent in the ethnic group also cause the disease to manifest. To add to the likelihood of this being the case, it has been determined that certain CYP genes are associated with predisposition to develop Lynch Syndrome. The polymorphism CYP1B1 rs1056836 CC—which was discussed above—is associated with CRC due to Lynch Syndrome (Kamiza et al., 2017). Since the product of this gene modulates metabolism and clearance of taxane chemotherapeutics and other anticancer drugs, understanding the workings of the gene is crucial in facilitating proper dosage during cancer treatment for Romanies. Worse yet, Kamiza et al. found that some of the markers associated with Lynch Syndrome display an interaction effect with meat consumption and cigarette smoking. CYP1B1 rs1056827 is one of them (Kamiza et al., 2017). This polymorphism has been associated with primary congenital glaucoma in Romanies in the past (Sivadorai et al., 2008). It is unclear how common this polymorphism is in the Romani population as a whole; regardless, because Romanies eat a diet high in meat and are also more likely to smoke than the average American, it would be beneficial to determine the incidence of this allele in Romani-American populations. Ways to Alleviate Cultural Misunderstanding in HealthcareIt is possible that a significant amount of the tension between Romani patients and their non-Romani providers could be alleviated with careful attention to transparency regarding medical procedures. This applies not only to the patients, but also their family members. Because family approval is required for all procedures, it is sensible to run each option by the members of the family who are with the patient, especially the elders. If it is a Romani-American woman, this especially holds true with her spouse. All possible consequences and side effects of each treatment option should be clarified, especially when looking at severe treatment options like chemotherapy. Potential drug interactions should be explained to the family as well so that they do not mix homemade natural remedies with conventional medicine in a harmful way. It is important for the provider to try not to be frustrated with the family if they ask many questions. Romani patients may be wary of gynecological diagnostic and routine wellness procedures such as pap smears due to the ethnic group’s recent history with sterilization. Explain why these procedures are important, and reassure them that there is purpose to conducting them. If possible, for women, have healthcare providers who are also women conduct any physical exams; the same holds true for men with healthcare providers who are also men. In the exam room, an understanding of Romani purity standards is key to optimal comfort for the patient. It is critical to avoid any form of contact between the top and bottom halves of the patient’s body during physical examination. This includes changing nitrile gloves between touching the halves of the body, giving two or more soap bars for patients to shower with, multiple towels with which to dry the body after a shower, and providing the patient with two-part hospital wear instead of gowns or robes. Sanitization materials for the furniture and bathroom should be provided as well. Perhaps paper/plastic disposable dishware and cutlery instead of reused ones from the hospital cafeteria would also be helpful, though Romanies may try to bring food from home into the hospital. If they do, providers should try to educate them as to why this is not appropriate, especially if the patient is immunocompromised, as is often the case with a cancer patient. The family will try to stay with the patient. If there are larger rooms for patients in the hospital, so long as resource allocation is fair to other patients and it does not take away from another patient in need, perhaps it would be helpful to give those rooms to the Romanies. If this is not possible, providing additional seating areas such as extra chairs to the family would make their stay easier, since many of them will want to be with the patient, especially if he or she is close to death. ConclusionsIt is important to keep in mind that Romanies are not a homogeneous group of people. As discussed above, they split off into many different tribes early on; each of those tribes settled in distinct regions and experienced different evolutionary pressures. For that reason, a limitation of any study trying to discuss Romani health is that different groups of Romanies might have very different genetic factors and experiences with healthcare that contribute to their outcomes. A way to help Romanies have better experiences as inpatients would be to require brief Romani cultural sensitivity training at hospitals serving a significant population of Romani-Americans. Desired results would include respect for purity standards to increase trust levels (such as changing gloves when moving between the upper and lower halves of the body). Such cultural sensitivity training should additionally lead to increased efforts to accommodate togetherness of the Romani-American inpatient’s family. Finally, knowledge of Romani mistrust of healthcare should lead providers to exhibit high levels of transparency regarding medical procedures. Doing so would relieve apprehension for the patients and help develop trust. The effects of cultural sensitivity training on healthcare providers’ attitudes, as well as health outcomes for patients, have been investigated in the past. Providers with such training have a better understanding of multiculturalism, show a significant improvement in cultural awareness, are more likely to consider social circumstances and show appreciation for importance of culture, and are more likely to adopt related ideas proposed in healthcare literature than providers who do not receive training (Majumdar et al., 2004). Meanwhile, patients seen by trained healthcare providers report greater overall functioning capacity and lower total health and social expenditures, with $11,000 compared to $18,000 at baseline 1.5 years after the training took place (Majumdar et al., 2004). Increased social support to Romani-Americans could carry more of them through school. Creating schooling programs with curricula that do not conflict with Romani culture may help more of them learn about the consequences of unhealthy lifestyle and dietary choices, such as obesity and smoking. Romanies have been shown to be responsive to education regarding healthcare practices if it is presented in a way that is palatable to them (Thomas, 1985). Since Romanies eat a large amount of red meat, and because they are more likely to smoke, improved understanding of interactions between these behaviors and diseases (such as Lynch Syndrome) could help them make better choices to facilitate positive long-term health outcomes. On the biological side, additional research is necessary on genetic patterns and possible syndromes leading to deadly cancers in Romanies. For American healthcare providers, this is especially true regarding research of Romani-Americans, as genetic patterns of Romanies in America may differ from those in the studies conducted in Eastern Europe, where most of the studies we have today were conducted. Understanding other genetic predispositions to cancer and chronic disease in Romanies could help both them and their healthcare providers pay special attention to changes in health that resemble signs of cancer, improving the likelihood of early detection and bettering chances of survival. Additionally, screening for polymorphisms in CYP genes and others could lead to more efficient dose-response ratios in chemotherapy. Knowing more about genetic predispositions to cancer could also help us find ways to prevent genetic cancers from appearing. Between CYP, PRDM, LAMB, and others that have been mentioned in this paper, there are a variety of genes that have been identified in Romanies that could potentially have malignant effects. There are still others which do not necessarily link to cancer, but lead to other adverse health outcomes for people in this ethnic group. If we understand more about these genetic predispositions to cancer and other chronic disease, such as incidence, resulting disease penetrance, and how it is inherited, many lives can be saved. This is especially important considering the consanguinity present in Romani culture, and how the people’s travelling nature can lead to the founder effect propagating disease. Screening—such as colonoscopies, endoscopies, pap smears, biopsies, blood tests, and carrier testing—could assist in detecting these diseases in their early stages or in their genotypes, before they have a chance to harm the patient. Newborn screening could also detect genetic issues in Romani children before they have a chance to manifest, allowing parents to take necessary precautions to help their children live healthy, fulfilling lives (Kalaydijeva et al., 2001). A possible solution would be to make this testing more available to Romani-Americans, not only by offering it directly to their communities, but by educating healthcare professionals to understand their culture and help build the trust necessary to facilitate compliance. Romanies are not the only ethnic group that has suffered from rare diseases related to genetic phenomena. The Finns, Jewish people, and French Canadians have been researched for similar instances, as well; unlike those groups, however, Romanies have not benefitted from the results of research on them (Kalaydijeva et al., 2001). If more attention from geneticists, healthcare professionals, and policymakers were directed to this too-often overlooked ethnic group, perhaps we will see a brighter future for them. ReferencesBodner, A., & Leininger, M. (1992). Transcultural Nursing Care Values, Beliefs, and Practices of American (USA) Gypsies. Journal of Transcultural Nursing, 4(1), 17-28. doi:10.1177/104365969200400104 Bradford, A. (2017, January 16). Roma Culture: Customs, Traditions & Beliefs. Live Science. Retrieved April 15, 2018, from https://www.livescience.com/44512-gypsy-culture.html/ Brennan, S. (2017). Gypsy boy, 13, who's been forced out of ELEVEN schools claims teachers are more prejudiced than pupils - and one excluded him from class as she didn't feel “comfortable” teaching him. The Daily Mail. Retrieved April 15, 2018, from http://www.dailymail.co.uk/femail/article-4906296/Gypsy-boy-13-forced-ELEVEN- schools.html#ixzz5BGfiIZr5 Browning, B. L., & Browning, S. R. (2013). Improving the Accuracy and Efficiency of Identity- By-Descent Detection in Population Data. Genetics, 194(2), 459-471. doi:10.1534/genetics.113.150029 Courbet, M., Fontenot, H. J., Hancock, I. F., & Sabata-Keplinger, M. (1996). The Patrin Web Journal: Romani Culture and History. Retrieved from http://www.oocities.org/~patrin/B ibliography de la Chapelle, A. (2004). Genetic Predisposition to Colorectal Cancer. Medscape. Retrieved April 15, 2018, from https://www.medscape.com/viewarticle/491394 Expression of LAMB3 in Cancer - Summary. (n.d.). The Human Protein Atlas. Retrieved from http://www.proteinatlas.org/ENSG00000196878-LAMB3/pathology Gheorghe, N. (1991). Roma-Gypsy Ethnicity in Eastern Europe. Social Research, 58(4), 829- 844. Retrieved from http://www.jstor.org.ezproxy.lib.utexas.edu/stable/40970676 Gross, J. A., Miller, Z., Pennington, M., Lidman, M., . . . Blum, M. (2018). Pig farm to be removed from Roma Holocaust site. Times of Israel. Retrieved from https://www.timesofisrael.com/pig-farm-to-be-removed-from-roma-holocaust-site/ Hajioff, S., & McKee, M. (2000). The health of the Roma people: a review of the published literature. Journal of Epidemiology & Community Health , 54(11), 864-869. Hancock, I. F. (2010). Roma (Gypsies). Austin, TX: Handbook of Texas Online. Hancock, I. F. (2010). We Are the Romani People: Ame Sam le Rromane Džene. Hatfield: University of Hertfordshire Press. Hancock, I. F. (2010). “Origins,” in Karanth, Dileep, ed., 2010. Danger! Educated Gypsy. Selected Essays by Ian Hancock. Hatfield: University of Hertfordshire Press. Hancock, I. F. (2016). “Romani.” In Delyn Day, Poia Rewi & Rawina Higgins, eds., The Journey of Besieged Languages, Newcastle: Cambridge Scholars Press. Hebbard, L., & Ranscht, B. (2014). Multifaceted roles of Adiponectin in Cancer. Best Practice & Research Clinical Endocrinology & Metabolism, 28(1), 59-69. doi:https://doi.org/10.1016/j.beem.2013.11.005 Hoefling, L. (2017, September 18). Where the Sidewalk Ends and PC Begins…. Retrieved May 4, 2018, from http://larryhoefling.com/blog/where-the-sidewalk-ends-and-pc-begins/ Kalaydjieva, L., Gresham, D., & Calafell, F. (2001). Genetic studies of the Roma (Gypsies): A review. BMC Medical Genetics, 2(1). doi:10.1186/1471-2350-2-5 Kamiza, A. B., You, J., Wang, W., Tang, R., Chang, C., Chien, H., . . . Yeh, C. (2017). Polymorphisms of xenobiotic-metabolizing genes and colorectal cancer risk in patients with lynch syndrome: A retrospective cohort study in Taiwan. Environmental and Molecular Mutagenesis, 59(1), 69-78. doi:10.1002/em.22113 Krueger, P. M., Tran, M. K., Hummer, R. A., & Chang, V. W. (2015). Mortality Attributable to Low Levels of Education in the United States. Plos One, 10(7). doi:10.1371/journal.pone.0131809 Laayouni, H., Oosting, M., Luisi, P., Ioana, M., Alonso, S., Ricano-Ponce, I., . . . Netea, M. G. (2014). Convergent evolution in European and Rroma populations reveals pressure exerted by plague on Toll-like receptors. Proceedings of the National Academy of Sciences, 111(7), 2668-2673. doi:10.1073/pnas.1317723111 Lutz, B. D. (1995). Gypsies as Victims of the Holocaust. Holocaust and Genocide Studies, 9(3), 346-359. doi:10.1093/hgs/9.3.346 Lynch, H. (1999). Colorectal cancer and the Muir-Torre syndrome in a Gypsy family: A review. The American Journal of Gastroenterology, 94(3), 575-580. doi:10.1016/s0002-9270(98)00799-0 Majumdar, B., Browne, G., Roberts, J., & Carpio, B. (2004). Effects of Cultural Sensitivity Training on Health Care Provider Attitudes and Patient Outcomes. Journal of Nursing Scholarship, 36(2), 161-166. doi:10.1111/j.1547-5069.2004.04029.x Martínez-Cruz, B., Mendizabal, I., Harmant, C., Pablo, R. D., Ioana, M., Angelicheva, D., Comas, D. (2015). Origins, admixture and founder lineages in European Roma. European Journal of Human Genetics, 24(6), 937-943. doi:10.1038/ejhg.2015.201 Mayer, B., Silló, P., Mazán, M., Pintér, D., Medvecz, M., Has, C., . . . Kárpáti, S. (2016). A unique LAMB3 splice-site mutation with founder effect from the Balkans causes lethal epidermolysis bullosa in several European countries. British Journal of Dermatology, 175(4), 721-727. doi:10.1111/bjd.14646 Melegh, B. I., Banfai, Z., Hadzsiev, K., Miseta, A., & Melegh, B. (2017). Refining the South Asian Origin of the Romani people. BMC Genetics, 18(1). doi:10.1186/s12863-017-0547-x Muir-Torre Syndrome. (2014, December 10). Cancer.Net. Retrieved April 15, 2018, from https://www.cancer.net/cancer-types/muir-torre-syndrome Mukherjee, S. (2010). The Emperor of All Maladies. NY: Scribner. Nagy, A., Sipeky, C., Szalai, R., Melegh, B. I., Matyas, P., Ganczer, A., . . . Melegh, B. (2015). Marked differences in frequencies of statin therapy relevant SLCO1B1 variants and haplotypes between Roma and Hungarian populations. BMC Genetics, 16(1). doi:10.1186/s12863-015-0262-4 Nagy, A., Szalai, R., Magyari, L., Bene, J., Toth, K., & Melegh, B. (2015). Extreme differences in SLCO1B3 functional polymorphisms in Roma and Hungarian populations. Environmental Toxicology and Pharmacology, 39(3), 1246-1251. doi:10.1016/j.etap.2015.04.019 National Institute of Health. (n.d.). Cytochrome P450 - Genetics Home Reference. Retrieved April 15, 2018, from https://ghr.nlm.nih.gov/primer/genefamily/cytochromep450 Omran, A. R. (2005). The Epidemiologic Transition: A Theory of the Epidemiology of Population Change. Milbank Quarterly, 83(4), 731-757. doi:10.1111/j.1468-0009.2005.00398.x Ostendorf, A. (2013). Roma Americans. In C. E. Cortés (Ed.), Multicultural America: A Multimedia Encyclopedia (Vol. 1, pp. 1849-1851). Thousand Oaks, CA: SAGE Publications Ltd. doi: 10.4135/9781452276274.n749 Petrášová, D., Bertková, I., Petrášová, M., Hijová, E., Mareková, M., Babinská, I., . . . H. (2014). Biomarkers Associated with Obesity and Overweight in the Roma Population Residing in Eastern Slovakia. Central European Journal of Public Health, 22(Supplement). doi:10.21101/cejph.a3896 Saison, C., Helias, V., Ballif, B. A., Peyrard, T., Puy, H., Miyazaki, T., … Arnaud, L. (2012). Null alleles of ABCG2 encoding the breast cancer resistance protein define the new blood group system Junior. Nature Genetics, 44(2), 174–177. http://doi.org.ezproxy. lib.utexas.edu/10.1038/ng.1070 Sedláková D. (2014). Low Socioeconomic Status and Unhealthy Lifestyle Lead to High Morbidity in Young Roma of East Slovakia. Central European Journal of Public Health, 22(Supplement). doi:10.21101/cejph.a4008 Silverstein, S. (1974). Where the Sidewalk Ends: The Poems & Drawings of Shel Silverstein (pp. 50). New York: Harper and Row. Sipeky, C., Weber, A., Szabo, M., Melegh, B. I., Janicsek, I., Tarlos, G., . . . Melegh, B. (2013). High prevalence of CYP2C19*2 allele in Roma samples: study on Roma and Hungarian population samples with review of the literature. Molecular Biology Reports, 40(8), 4727-4735. doi:10.1007/s11033-013-2569-4 Sivadorai, P., Cherninkova, S., Bouwer, S., Kamenarova, K., Angelicheva, D., Seeman, P., . . . Kalaydjieva, L. (2008). Genetic heterogeneity and minor CYP1B1 involvement in the molecular basis of primary congenital glaucoma in Gypsies. Clinical Genetics, 74(1), 82-87. doi:10.1111/j.1399-0004.2008.01024.x Stewart, M. (1997). 12: The Shame of the Body. In The Time of the Gypsies (pp. 204- 231). Boulder, CO: Westview Press. Retrieved from Anthropology Online database. Stoyanova, G. (2013). Romedia Foundation. Forced sterilization of Romani women – A Persisting Human Rights Violation. Retrieved February 25, 2018, from https://romediafoundation.wordpress.com/2013/02/07/forced-sterilization-of-romani-women-a-persisting-human-rights-violation/ Strochlic, N. (2013, December 22). American Gypsies Are a Persecuted Minority That Is Starting to Fight Back. The Daily Beast. Retrieved from https://www.thedailybeast.com/ american-gypsies-are- a-persecuted-minority-that-is-starting-to-fight-back Sutherland, A. (1992). Cross-Cultural Medicine, A Decade Later: Gypsies and Health Care. Western Journal of Medicine, 157(3), 276-280. Szalai, R., Hadzsiev, K., & Melegh, B. (2016). Cytochrome P450 Drug Metabolizing Enzymes in Roma Population Samples: Systematic Review of the Literature. Current Medicinal Chemistry, 23(31), 3632-3652. doi:10.2174/0929867323666160809092455 Thomas, J. D. (1985). Gypsies and American Medical Care. Annals of Internal Medicine, 102(6), 842. doi:10.7326/0003-4819-102-6-842 Thomas, J. D., Doucette, M. M., Thomas, D. C., & Stoeckle, J. D. (1987). Disease, Lifestyle, And Consanguinity In 58 American Gypsies. The Lancet, 330(8555), 377-379. doi:10.1016/s0140-6736(87)92392-0 Tsuruta, D., Kobayashi, H., Imanishi, H., Sugawara, K., Ishii, M., & Jones, J. (2008). Laminin-332-Integrin Interaction: A Target For Cancer Therapy? Current Medicinal Chemistry, 15(20), 1968-1975. doi:10.2174/092986708785132834 U.S. Census Bureau (2015). 2011-2015 American Community Survey 5-Year Estimates. Retrieved from https://factfinder.census.gov/faces/tableservices/jsf/pages/productvi ew.xhtml?pid=ACS_15_SPT_B01003&prodType=table. Van der Zee, R. (2016, July 19). Roma women share stories of forced sterilisation. Al Jazeera. Web. VanSaun, M. N. (2013). Molecular Pathways: Adiponectin and Leptin Signaling in Cancer. Clinical Cancer Research, 19(8). doi:10.1158/1078-0432.CCR-12-0930 Vivian, C., & Dundes, L. (2004). The Crossroads of Culture and Health Among the Roma (Gypsies). Journal of Nursing Scholarship, 36(1), 86-91. doi:10.1111/j.1547- 5069.2004.04018.x Weber, A., Szalai, R., Sipeky, C., Magyari, L., Melegh, M., Jaromi, L., . . . Melegh, B. (2015). Increased prevalence of functional minor allele variants of drug metabolizing CYP2B6 and CYP2D6 genes in Roma population samples. Pharmacological Reports, 67(3), 460- 464. doi:10.1016/j.pharep.2014.11.006 White, M. C., Babcock, F., Hayes, N. S., Mariotto, A. B., Wong, F. L., Kohler, B. A., & Weir, H. K. (2017). The history and use of cancer registry data by public health cancer control programs in the United States. Cancer, 123, 4969-4976. doi:10.1002/cncr.30905 
From the Inquiries Journal Blog   Monthly Newsletter SignupThe newsletter highlights recent selections from the journal and useful tips from our blog. Suggested Reading from Inquiries Journal
Inquiries Journal provides undergraduate and graduate students around the world a platform for the wide dissemination of academic work over a range of core disciplines. Representing the work of students from hundreds of institutions around the globe, Inquiries Journal's large database of academic articles is completely free. Learn more | Blog | Submit Follow IJ
Latest in Health Science |