Single-Payer Reform and Rural Health in the United States: Lessons from Our Northern Neighbor
By
2021, Vol. 13 No. 03 | pg. 1/1
IN THIS ARTICLE
KEYWORDS
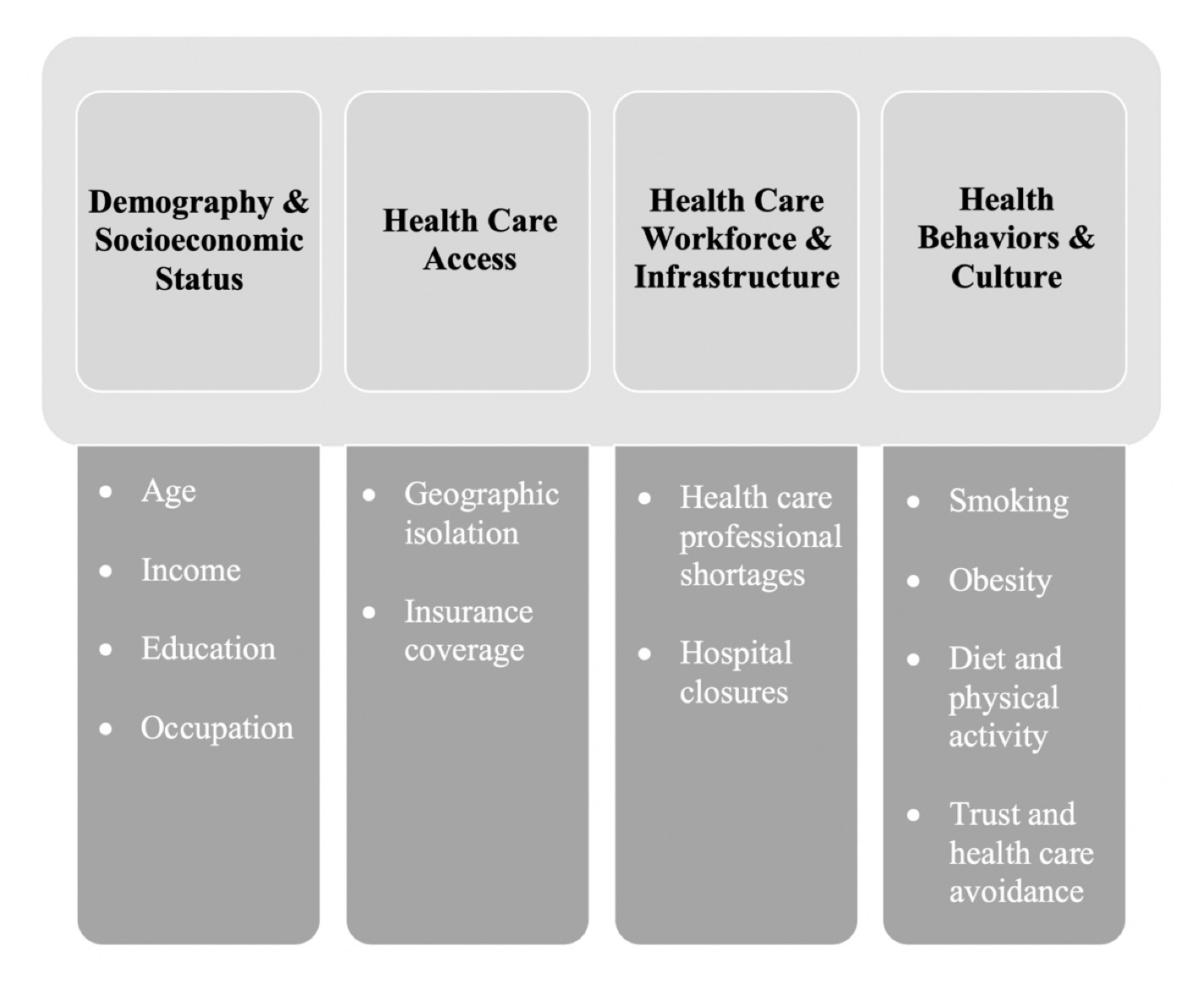
AbstractSingle-payer health reform has secured its place in the mainstream American health policy debate, yet its implications for particular subpopulations or sectors of care remain understudied. Amidst many unanswered questions from policymakers and political pundits, rural health has emerged as one such area. This article explores rural Canada’s five-decade-long experience with a national publicly funded health insurance program as a valuable opportunity for cross-national learning. During March 2020, I conducted 13 semi-structured, elite stakeholder interviews with government officials, academic researchers, rural hospital executives, public health association leaders, rural health administrators, and representatives from provincial medical, hospital, and physician associations in Ontario. I found that a single-payer model confers notable advantages over a market-based model, including improved rural hospital viability and enhanced governmental authority to plan health services. However, despite these advantages, advances in Canadian rural health care have remained modest, and those that have occurred seem to be derived as much from a basic value commitment to tackling rural health issues as from the structure of Canada’s single-payer model itself. These results suggest that designing a national single-payer program in the United States that successfully ameliorates geographic health disparities will require a specific and concerted focus on addressing rural health issues. In the absence of such a focus, any single-payer program instituted in the U.S. risks inadequately meeting the pressing and unique health care needs of rural communities. The national health care debate has once again taken center stage in the United States with voters citing health reform as the most important issue in the November 2020 presidential election (Gallup 2020). While the sentiment animating today’s conversation—a widespread dissatisfaction with the availability and affordability of health care—is nothing new, the menu of proposed reforms receiving serious consideration has shifted perceptibly. In the Democratic presidential nominating process of 2019 and 2020, a large group of contenders ventured beyond proposals to build on the Affordable Care Act and joined perennial health care “radical” Bernie Sanders in championing an ambitious government health insurance program dubbed “Medicare For All” (Keith 2019b). Bolstered by strong public opinion polling and the endorsement of elected officials at both the national and state levels, single-payer reform has secured its place in the mainstream American health policy debate (Lopes et al. 2020; Oberlander 2019). Amid an uproarious nominating process, Medicare For All became a rallying cry for Democratic politicians eager to prove the boldness of their policy vision and energize the progressive left wing of the party (Draper 2019). This discussion, however, dwelled on big-picture rhetorical themes, such as universal coverage and “health care as a right,” while largely neglecting the ground-level operational details of single-payer systems (Katz, Quealy, and Sanger-Katz 2019; Rochefort 2020).One area in which many questions remain is rural health. In the first Democratic primary debate in June 2019, former Representative John Delaney (D-MD) defended his opposition to Medicare For All with this explanation: “If you go to every hospital in this country and you ask them one question—which is ‘how would it have been for you last year if every one of your bills were paid at the Medicare rate?’—every single hospital administrator said they would close. . . . So, to some extent, we’re basically supporting a bill that will have every hospital close” (“Full Transcript” 2019). This comment generated a wave of confusion about the implications of a single-payer system for hospitals, particularly those in rural areas (Abelson 2019; Goldsmith and Leibach 2019; Luthi 2019; Luthra 2019; O’Dowd 2019; Tarlo 2019). Following an inconclusive round of pundit responses, the Washington Post named single-payer’s effect on rural hospitals one of “Democrats’ three key disputes about Medicare For All” (Stein 2019). The purpose of this article is to bring together the concurrent, if still disconnected, discussions of single-payer health reform and rural health care. A review of the health challenges facing rural America will be followed by an analysis of the successes and struggles of the Canadian health system in addressing geographic health disparities, including noteworthy service and payment innovations in different provinces. The article concludes with a discussion of lessons derived from the Canadian experience and opportunities that might exist in the arena of rural health with the adoption of a single-payer program in the United States. Rural Health in the United StatesToday, the urban mortality penalty of early American history has reversed, giving way to a stark rural mortality penalty (Cosby et al. 2008). Since the mid-1980s, residents of rural areas have suffered from all-cause mortality rates significantly higher than those experienced by metropolitan residents (Cosby et al. 2019; Fenelon 2013; Singh and Siahpush 2014b). Rural residents also face higher rates of cause-specific mortality, including cardiovascular mortality (Singh et al. 2019), maternal mortality (Kozhimannil et al. 2019), and suicide mortality (Rossen et al. 2018; Singh and Siahpush 2002). Singh and Siahpush (2014a) found that the life expectancies of rural and urban residents vary significantly, with the former living, on average, 2.4 fewer years (79.1 years vs. 76.7 years). The factors contributing to the rural health penalty in the United States are myriad and intersectional. Some impinge directly on the provision of health services, while others operate outside the traditional health care sphere, shaping the behavioral and cultural landscape of rural America. As illustrated in Figure 1, here the etiology of diminished rural health is separated into four distinct categories: demography and socioeconomic status, health care access, health care workforce and infrastructure, and health behaviors and culture.
Figure 1: Etiology of the American rural health penalty. Demography & Socioeconomic StatusRural residents are older than other Americans: 17.5% of the rural population is 65 years or older compared to 13.8% of the urban population, a difference that promises to grow even more drastic as the Baby Boomer cohort continues to age (Symens Smith and Trevelyan 2019). Older populations, more prone to develop health problems and often uninsured for particular illnesses or services (e.g., medications), pose obvious challenges for rural health care systems. Second, rural residents tend to be poorer and less educated than those living in or near urban centers, a phenomenon that has recently caught the attention of popular media in the U.S. (Booker 2018). The rural poverty rate (16.4%) outsizes that of urban areas (12.9%) by 3.5%, and the median household income of mostly urban counties ($59,970) eclipses that of mostly rural ($47,020) and completely rural ($44,020) counties by substantial margins (Guzman et al. 2018; USDA 2018). In 2015, less than one-third (28%) of rural adults held a postsecondary degree compared to 41% of urban adults, an achievement gap that has only grown since 2000 (USDA 2017). Unsurprisingly, recent research has linked the generally lower socioeconomic status of rural communities to increased rural mortality rates (Gong et al. 2019). Lastly, due to the organization of rural economies, rural residents are more likely to work in hazardous industries, such as agriculture, mining, forestry, and fishing, and thus stand at greater risk of work-related injuries and hospitalizations (Crosby et al. 2012: 10; Ricketts 2000). Health Care AccessAccess to health care in rural areas is limited by formidable physical and financial barriers. The low population density inherent to rural spaces makes traveling to receive health care a more difficult proposition. Geographic isolation has been associated with lower rates of preventive screening, less frequent treatment for chronic diseases and mental health problems, and higher rates of morbidity from acute and chronic conditions (Crosby et al. 2012: 8). The long distances between residents’ homes and health care centers, further complicated by limited access to vehicles, make transportation a major impediment to the receipt of acute and preventive care, resulting in increased rates of rescheduled or missed appointments, delayed care, and inconsistent medication use (Syed, Gerber, and Sharp 2013). Just as problematic as the physical barriers to care, though, are the financial. Americans living outside of a metropolitan statistical area (MSA) are more likely to be uninsured than those living within an MSA (13.8% vs. 10.2%) (CDC 2018). For ruralites who do have health insurance, public insurance—namely, Medicare and Medicaid—plays a critical role (Foutz, Artiga, and Garfield 2017). One report found that in 2014-2015, 45% of children and 16% of adults in rural areas were covered under Medicaid compared to 38% and 15%, respectively, in metropolitan areas (Wagnerman et al. 2017). The greater prevalence of individuals covered by Medicare and Medicaid, which pay providers less generously than private insurance (in many cases, less than the cost of care), contributes to the financial vulnerability of rural health care facilities (Daria 2018; Zuckerman, Skopec, and Epstein 2017). Health Care Workforce & InfrastructureRural communities face long-standing shortages of health care providers and facilities (Ricketts 2005; Rosenblatt and Hart 2000). Despite being home to about 20% of the American population, rural areas are home to only 9%, 15.6%, and 15.5% of the nation’s physicians, nurse practitioners, and physician assistants, respectively (Petterson et al. 2013). Almost all (85%) rural counties in the U.S. at some point have been classified by the Health Resources and Services Administration (HRSA) as primary care Health Professional Shortage Areas (Doescher et al. 2009). Accompanying the scarcity of rural health care providers has been a decline in the number of rural hospitals (Frakt 2019; Kaufman et al. 2016). According to the North Carolina Rural Health Research Program (n.d.), which tracks rural hospital closures nationwide, 135 rural hospitals have closed since January 2010, and another 673 rural hospitals remain financially vulnerable (iVantage 2016). As noted above, the precarious financial standing of rural hospitals stems in large part from rural America’s distinct demographic profile—that is, a concentration of older, poorer, and disproportionately uninsured and publicly insured patients. The consequences of hospital closures reach far and wide. For one, rural hospital closures are associated with reductions in local primary care and specialist physician workforces (Germack, Kandrack, and Martsolf 2019; Hart, Pirani, and Rosenblatt 1994). Facility closures also impact the health behaviors and outcomes of rural residents, exacerbating the propensity of rural residents to delay or forgo medical care and increasing overall mortality (Gujral and Basu 2019; Wishner et al. 2016). Given the pivotal role of rural hospitals as venues of both medical and economic activity, their closure also imposes financial costs on the communities they serve, reducing per-capita incomes by as much as $700 and increasing local unemployment rates by up to 1.6% (Holmes et al. 2006; Mandich and Dorfman 2017). The diffusion of innovations, such as telemedicine, that aim to improve access by circumventing entrenched workforce and infrastructure deficiencies has been stymied by additional challenges. Almost 30% of rural areas in the U.S. are without fixed terrestrial broadband internet, and nearly 60% of non-metro health care facilities lack adequate internet connectivity (FCC 2019; Whitacre, Wheeler, and Landgraf 2017). The lack of insurance parity laws for telehealth services further hinders implementation of such technologies since coverage varies widely by carrier and plan (Yang 2016). Health Behaviors & CultureOther factors driving the rural health penalty lie outside the realm of medical care. On the whole, rural Americans exhibit more health-harming behaviors and fewer health-protective behaviors than other Americans (Anderson et al. 2015; Matthews et al. 2017). Rural communities have higher rates of smoking (Atkins, Kim, and Munson 2017; Meit et al. 2014) and obesity (Befort, Nazir, and Perri 2012), as well as lower rates of physical activity (Parks, Housemann, and Brownson 2003; Reis et al. 2004) and poorer dietary habits (Sharkey, Johnson, and Dean 2011). This dangerous combination of behaviors, along with poor access to preventive care, contributes to high rates of chronic diseases, such as diabetes (Hale, Bennett, and Probst 2010). Often, a hesitance to engage with the health care system is also at play in rural communities. Spleen et al. (2014: 86) found a higher prevalence of health care avoidance in rural areas, seemingly instigated by “stigma, lack of privacy, lack of culturally appropriate interventions, and acceptance of poor health.” Especially among rural minority communities, trust in health care professionals is lacking, thanks, at least in part, to the inter-generational trauma inflicted by injustices such as the Tuskegee syphilis experiment of the mid-1900s (Barry-Jester 2017). Finally, a cultural emphasis on independence and self-reliance in rural America colors rural residents’ outlook on governmental assistance and social welfare (Osgood 1977). Any balanced discussion of rural culture, however, would be remiss should it overlook its protective elements. Rural communities enjoy a greater degree of social capital and a heightened sense of resilience and resourcefulness relative to urban centers (Crosby et al. 2012: 15-18; Hofferth and Iceland 1998). In light of research associating greater community social capital with improved population health, the social cohesion of rural communities likely serves to moderate the rural health penalty, albeit without eliminating it completely (Folland 2007). Rural Health Policy in the United StatesOver the past several decades, rural health policies have been implemented with the goal of alleviating geographic health disparities. Considering the United States’ failure to meet any of the rural mortality rate targets set by Healthy People 2020, the efficacy of these policies is questionable (Yaemsiri et al. 2019). Policies aimed at improving rural health care access have focused primarily on addressing transportation and insurance challenges. While all state Medicaid programs cover non-emergency medical transportation (NEMT) services, which assist residents who lack reliable transportation in attending medical appointments, some states require prior authorization and many have instituted limits and restrictions (KFF 2018). “Original” Medicare (i.e., Parts A and B), on the other hand, only covers NEMT where deemed “medically necessary” by a physician, essentially precluding reimbursement for transportation coverage to preventive care (CMS n.d.). The rural uninsurance problem was most recently targeted by the ACA’s extension of Medicaid eligibility to low-income adults, which disproportionately benefited rural residents in terms of coverage uptake (Benitez and Seiber 2018). Between 2013 and 2015, expansion states saw hospitals’ uncompensated care costs fall by 1.6 percentage points (3.9% to 2.3%), amounting to a total savings of $6.2 billion (Dranove, Garthwaite, and Ody 2017). However, the Supreme Court’s ruling in National Federation of Independent Business v. Sebelius striking down the ACA’s mandatory Medicaid expansion provisions made it such that these improvements have been enjoyed only by a subset of states. Over the same period, uncompensated care costs for hospitals in non-expansion states declined by only 0.3-0.4 percentage points, and rural hospitals in non-expansion states are now five times more likely to close than those in expansion states (Dranove, Garthwaite, and Ody 2017; Lindrooth et al. 2018). Further complicating matters, the clustering of non-expansion states in the South, a region home to over 90% of rural Blacks and 58% of Blacks nationwide, has led researchers to point to the racialization of Medicaid expansion as evidence of systemic racism at work in American rural health care (Grogan and Park 2017; Hirschfield 2019; Kozhimannil and Henning-Smith 2018). While the expansion gap (and the tangle of racial and political factors driving it) is problematic, what may be most concerning is the ongoing legal threat to the ACA, as Texas v. United States—which has the potential to strike down the statute in its entirety—makes its way through the federal court system (Keith 2019c). In terms of rural health care workforce and infrastructure, existing policies focus on correcting for the inequitable distribution of physicians and promoting the financial stability of select facilities. To incentivize physicians to practice in medically underserved areas, the National Health Service Corps offers loan repayment and scholarships in return for at least two years of service in a Health Professional Shortage Area (HRSA n.d.). Other programs to financially incentivize and/or academically support rural practice exist at the state and local levels (AAMC n.d.). Additionally, some physician shortages are filled by foreign medical graduates permitted to practice in the United States through J-1 visas, which require that these physicians work in medically underserved areas (Baer et al. 1998). The financial challenges of rural medical facilities are a major target of federal rural health policy. More than half (54%) of rural hospitals are designated by CMS as Critical Access Hospitals (CAHs), hospitals that must meet certain criteria, including location in a rural area more than 35 miles from another hospital (15 miles in areas with rough terrain) and a bed count of no more than 25 (Flex Monitoring Team n.d.; MACPAC 2018). Because the low population density and higher health care costs associated with rural health care make traditional fee-for-service models unsustainable, Medicare pays CAHs through cost-based reimbursement, covering 101% of their cost for treating Medicare patients (MACPAC 2018). The alternative payment structure for CAHs has been shown to improve hospital financial performance and longevity (Li, Schneider, and Ward 2009). Federally-qualified health centers (FQHCs) and rural health clinics (RHCs) are also major players in the health care landscape of rural areas, with one in five rural residents relying on a HRSA-funded health center for their care (HRSA n.d.). Operating under a mandate to provide comprehensive primary care services to medically underserved areas/populations regardless of patients’ means, FQHCs are paid by CMS according to a payment schedule based either on a locally-adjusted national rate (Medicare) or on the average rates of geographically proximate clinics (Medicaid) (CMS 2019; MACPAC 2017). RHCs receive enhanced reimbursement from CMS through similar alternative payment schemes. While these publicly funded facilities serve as lifelines for many rural residents, targeted programs have their limits. Over 660,000 Americans today live in rural counties without an FQHC, RHC, or acute care hospital (Clawar et al. 2018). Additional payment reforms have been implemented to support rural health care facilities. Disproportionate Share Hospital (DSH) payments provide supplementary payments to hospitals serving large low-income populations. Under the ACA, DSH payments were to be gradually phased out between 2014 and 2020 under the assumption that the financial burden for which they were compensating would be alleviated by the increased coverage associated with universal Medicaid expansion. The ensuing uneven adoption of Medicaid expansion has left rural hospitals in non-expansion states heavily reliant on DSH payments, and scheduled cuts have been delayed by Congress each year since 2012 (Keith 2019a). Research examining the potential implications of future DSH payment cuts has found that such cuts would severely threaten the financial stability of safety-net hospitals, almost half (42.5%) of which are already in weak financial condition (Cole et al. 2014; Neuhausen et al. 2014). One-off state innovations have emerged as a sort of natural experimentation for solving rural health challenges. In 2017, the CMS Innovation Center announced $25 million of funding for a rural health care pilot program in Pennsylvania (CMS Innovation Center n.d.). Under this initiative, the 13 participating rural hospitals operate with global budgets and are subject to performance targets to incentivize improvement in quality and coordination of care. Further research is required to characterize the potential of this Canada-style global hospital budgeting for rural health care in the United States. Canadian Health Care: A Rural PerspectiveOf all international health care systems, the Canadian health care system is the most frequently referenced by American politicians and arguably the best understood by the American public. Yet, fundamental misconceptions have endured, including those surrounding the role of government in delivering services, the comprehensiveness of the public insurance plan, and the respective political responsibilities of the federal and provincial governments. While Canada’s publicly funded health care system, Medicare, operates under a single-payer model that provides every Canadian with basic health care coverage, it does not cover all health services and leaves the delivery of services to private providers. Canadian health care financing falls into three distinct “layers,” each providing different levels of coverage (Martin et al. 2018; Rochefort 2020). Medically necessary hospital, diagnostic, and physician services, which comprise the first layer, are completely covered by Medicare. Services occupying the second layer, such as outpatient prescription drugs, mental health care, and long-term institutional care, are covered on a variable basis across the provinces and territories, while third-layer services (e.g., dental care, routine eye care, outpatient physical therapy) are typically not covered at all. The Canadian government pays for roughly 70% of total health expenditures with the remainder covered by private insurance and out-of-pocket payments (CIHI 2019). The administration of the program and the bulk (76%) of its costs rest with the 13 provincial and territorial governments (Allin and Rudoler 2017). As long as their programs meet the five core principles laid out in the Canada Health Act of 1984 (accessibility, universality, portability, comprehensiveness, and public administration), the provinces have largely independent authority over planning the provision of health services and expanding or cutting “second-layer” benefits, the principle exception being the federal government’s role in providing care to special populations (e.g., military personnel, indigenous populations) (Blankenau 2010). This strong federalism component, reflecting the classic tensions of intergovernmental relations, makes Canada’s health care system function much more like 13 independent health insurance plans than one unified national plan (Fierlbeck 2011: 54–55). To appreciate the central role of rural health in shaping the motivations and objectives of Medicare from the outset, the origins of the program must be examined. Publicly funded health care in Canada was pioneered by Saskatchewan, one of three rural “Prairie Provinces.” As early as 1916, rural municipalities in Saskatchewan were laying the groundwork for public health care financing, cooperating to form Union Hospital Districts to construct and operate rural hospitals. When the Great Depression hit the Prairie Provinces, leaving many agricultural communities unable to afford health care and threatening the survival of local hospitals, the dominant public-private hospital financing model “failed miserably,” while rural Saskatchewan’s public model “proved quite resilient” (Ostry 2012: 22). Extensive grassroots organizing and the election of North America’s first socialist government facilitated the province-wide expansion of this public model via the 1947 Saskatchewan Hospital Insurance Plan (Jones 2019: 111–19). An almost identical iteration of this policy cycle transpired in the next decade, culminating with the passage of the Saskatchewan Medical Care Insurance Act in 1962, four years prior to the national adoption of a public health insurance plan with the Medical Care Act of 1966. The unique challenges posed by rural health care were the impetus for Saskatchewan’s public health care financing plans, and thus a driver of the national programs that followed; however, while the development of Canada’s single-payer system certainly improved access to health care services for rural residents, improved access has not translated to equitable access. Today, geographic health disparities (in addition to racial and socioeconomic inequities), fueled by factors practically identical to those fueling similar disparities in the United States (Figure 1), persist in the face of universal coverage (Frohlich, Ross, and Richmond 2006; PHAC 2018). Most tellingly, rural Canadians suffer from higher rates of preventable mortality and a lower life expectancy compared to their non-rural counterparts (CIHI 2006; Subedi, Greenberg, and Roshanafshar 2019). Medicare’s inability to more substantially reduce or eliminate geographic health disparities despite its rural roots contextualizes and justifies the contemporary evaluation of Canada’s single-payer system through a rural health lens. The following discussion of rural health and rural health policy in Canada is based on a research visit by the author to the province of Ontario (Toronto and Ottawa) in March 2020, during which 13 semi-structured, elite stakeholder interviews were conducted with government officials, academic researchers, rural hospital executives, public health association leaders, rural health administrators, and representatives from provincial medical, hospital, and physician associations. To supplement these interview findings, relevant academic and popular literature—including scholarly publications, government and nonprofit reports, and news articles—was consulted. Canadian Rural Health PolicyThe challenges of rural health were thrust into the mainstream Canadian health policy debate in December 2002 with the release of the final report of the Commission on the Future of Health Care in Canada, commonly known as the Romanow Report. Referencing urban-rural disparities in life expectancy, infant mortality, and all-cause mortality rates, the Romanow Report found that “geography is, in fact, a determinant of health” (Commission on the Future of Health Care in Canada 2002: 159). Concluding its section on rural health, the report declared: “Currently there is no coherent national approach for addressing issues specific to rural communities” (Commission on the Future of Health Care in Canada 2002: 159). The absence of a “coherent national approach” persists to date. Due to the division of governmental authority in Canada, practically all movement in rural health policy has taken place at the provincial level. In attempting to reduce the health penalty afflicting rural Canadians, provinces have concentrated their efforts on policies concerning physician distribution, hospital availability and accessibility, rural health services organization and planning, and telehealth coverage. Albeit modest, some pan-Canadian action on rural health issues has accompanied provincial efforts, particularly in recent years. Physician DistributionPolicies aimed at ameliorating urban-rural disparities in health workforce supply have focused on financial incentives for recruitment of physicians and allied health professionals. In 1997, a landmark case out of the Supreme Court of British Columbia (Waldman v. The Medical Services Commission of British Columbia, et al.) barred provinces from reducing reimbursement rates for physicians who settled in well-served areas, meaning health officials were “denied the sticks and left with the carrots in their physician supply strategies” (Fierlbeck 2011: 133). Since then, all provinces have offered programs to incentivize, with differing degrees of generosity, physicians to relocate to rural and remote communities. Rural-specific medical training has also been used to promote rural practice. In 2005, Ontario established a rural-centric medical school, the Northern Ontario School of Medicine, focused on recruiting “rural-born” students and training the next generation of rural physicians. The persistence of rural physician supply shortages, despite these policies, has frustrated rural stakeholders, some of whom feel that incentive programs have not addressed the “root causes” of the problem and have contributed to a self-perpetuating cycle of “band-aid” solutions (Grzybowski and Kornelsen 2013: 11). Hospital PolicyWith 22% of Canadians (roughly 7 million residents) living more than a one-hour drive from a Level I or Level II trauma center, rural hospital policy is very much an ongoing priority. The Canadian constitution delegates the establishment and maintenance of hospitals to the respective provincial governments. While provinces have dealt with hospital issues in different ways, the accessibility principle of the Canada Health Act has generally been interpreted to mean financial—not geographic—accessibility, suggesting that rural Canadians do not have a right to immediate access to health services, but rather access “where and as available” (Fleet et al. 2013: 191; Rechel et al. 2016). The ambiguity of this interpretation has sparked debate over the medically and financially optimal locations of rural hospitals. Some provinces, particularly in times of economic decline or stagnation, have opted to close, repurpose, or merge rural hospitals—or have at least threatened to do so. In the 1990s, facing rising health care spending, federal cutbacks to Medicare, and a severe budget deficit, Saskatchewan turned its cost-cutting sights on rural hospitals. During this period, 52 rural hospitals in the province were “closed,” 23 of which continued to receive funding to operate as long-term care facilities, and 29 of which were offered one-time funding to convert to primary care centers (James 1999). Although less than a handful of hospitals closed permanently, the public response was vociferous, with many Saskatchewanians viewing rural hospital closures as “death certificate[s]” for affected communities (1030). In Ontario, the Health Services Restructuring Commission (HSRC) of 1996-2000 studied the province’s rural hospitals and made recommendations for reform. Approaching rural, northern, and remote hospitals differently than large, urban hospitals, the Commission released a rural health care framework that centered on the creation of Rural and Northern Health Care Networks, each composed of multiple hospitals offering varying levels of acute care (OMHLTC 1998; Sinclair, Rochon, and Leatt 2005: 1). Sixteen of these networks were designed by the Commission, but the prospect of political backlash in rural ridings prompted the government to stop short of mandating their establishment (108–9). The rural and northern components of the HSRC, while more aspirational than material, set the stage for Ontario’s subsequent experimentation with rural integrated care models. Health Services PlanningAs suggested by the saga of Ontario’s HSRC, innovation in the organization of health services has been central to Canada’s rural health care strategy. In many provinces, this innovation has taken the form of regionalization or districting. While decentralized management theoretically helps to tailor the delivery and organization of services to the needs of each district, without an explicit focus on rural health and depending on the composition of the catchment areas/populations, even localized bodies risk overlooking the concerns of rural residents. For instance, out of the 12 Local Health Integration Networks (LHINs) in southern Ontario, only one developed a rural-specific strategy (Whaley 2020). Ontario has experimented with rural-specific health models on a provincial level, however. In 2016, the Ontario Ministry of Health and Long-Term Care (OMHLTC) announced an investment of 2.5 million CAD in the creation of Rural Health Hubs at five health care centers around the province (Office of the Premier 2016). Rural Health Hubs integrated inpatient, outpatient, mental/behavioral, and long-term health care under a single funding envelope, in addition to contracting with “peripheral” health services (e.g., public health, ambulance services) and partnering with community organizations for the provision of social services, recreation, and education (Multi-Sector Rural Health Hub Advisory Committee 2015). Despite being well-received by the Ontario Hospital Association, the pilot program never expanded beyond the initial five Hubs. The election of a new Conservative provincial government in 2018 resulted in the creation of a new initiative, Ontario Health Teams, which replaced both the LHINs and Rural Health Hubs and raised concerns about the trajectory of rural health reform in the province. With many final design details, such as the budgeting methodology and the size of the catchment areas/populations, still to be determined, it is unclear how Ontario Health Teams will improve rural health care in the province, if at all. TelehealthThe ability of telehealth and other virtual care services to connect rural and remote Canadians with health care providers is cited by many rural stakeholders as key to the future of rural health care in Canada. Over the past two decades, telehealth has expanded rapidly, with the number of annual telehealth consultations nationwide predicted to reach more than one million in coming years (Nasser and Chen 2014). In Ontario, the number of annual telehealth visits increased more than eightfold between 2008 and 2014. With telehealth utilization higher and therapeutic areas of care more diverse in northern Ontario than in southern parts of the province, this increase has been particularly consequential for the health of rural and remote communities (O’Gorman, Hogenbirk, and Warry 2016). Unlike in the United States, telehealth is widely covered in Canada. Rural and remote residents are able to access these services at no extra cost through their provincial insurance plans. All provinces have designated telehealth billing codes, and some even pay additional fees to providers for delivering services through technology (Waddell, Scallan, and Wilson 2018). Pan-Canadian ActionAiming to bridge the gaps between provincial approaches and build a cohesive national approach to rural health, in 2017 the College of Family Physicians of Canada and the Society of Rural Physicians of Canada established the Rural Road Map for Action (Advancing Rural Family Medicine: The Canadian Collaborative Taskforce 2017a). Unlike provincial initiatives, which tend to target one particular challenge in rural health (e.g., physician supply, health sector models, etc.), the Rural Road Map has brought together the five “pentagram partners”—policymakers, health professionals, universities, health and education administrators, and community members—to improve the health of rural and remote Canadians across multiple dimensions (Advancing Rural Family Medicine: The Canadian Collaborative Taskforce 2017b). Not only has the initiative released actionable rural-centric recommendations, in January 2020 the Rural Road Map Implementation Committee released a scorecard detailing the current status of each recommendation (Wilson et al. 2020). While the establishment of an initiative as organized and progressive as the Rural Road Map is encouraging, the relatively static nature of pan-Canadian rural health policy must be acknowledged. In the recently published progress report, the architects of the Rural Road Map conclude: “Currently, there is no comprehensive national (or even provincial) rural health-care strategy to address the needs of the rural population”—a practically verbatim repetition of the Romanow Report’s conclusion almost two decades prior (Wilson et al. 2020: 17). Lessons From Our Northern NeighborAs Rochefort and Donnelly (2008: 132) eloquently noted, “If imitation is the sincerest form of flattery, then Canadians have good reason to feel rebuffed by their southern neighbors when it comes to healthcare reform.” Up until now, the United States has shied away from the Canadian example in health care policy, despite the advocacy of numerous scholars (Galvani et al. 2020; Seidman 2014; Woolhandler et al. 2003) and activist groups (e.g., Physicians for a National Health Program). Moreover, such discussions of cross-national learning as do occur have been limited, focusing either on macro-level indicators (e.g., costs and insurance coverage)—as exemplified by the General Accounting Office’s report on the lessons of the Canadian model (GAO 1991)—or on micro-level anecdotal comparisons of patient experiences, as depicted in Michael Moore’s popular documentary Sicko or in mainstream media reports (Abutaleb 2019). Meso-level studies like the one undertaken here, focusing on the implications of a Canada-style single-payer mechanism for particular subpopulations or sectors of care, can bridge this divide. Hospital ViabilityCanada’s single-payer model ensures the financial viability of small, rural hospitals—the sort of hospitals shuttered by the dozen in the U.S. over the past decade. While facilitated in part by universal coverage of the population under Medicare, the financial stability of rural hospitals in Canada is not solely a product of government-financed health insurance, but also the result of hospital financing policies intended to institutionalize a public commitment to access. Unlike in the U.S., where rural hospitals scramble to cover expenses from a hodgepodge of public and private payers, rural hospitals in Canada operating under global budgets can count on a constant (or even growing) annual disbursement from their provincial governments. Due to the demographic and socioeconomic composition of their patient populations as well as low patient volumes, small rural hospitals are inevitably more expensive and less efficient than other types of hospitals. Under a single-payer model in which the government has embraced the principle of universal access—as codified in the accessibility principle of the Canada Health Act, for instance—there is greater tolerance for the operational inefficiency of rural hospitals than is found in a largely market-driven system like that of the U.S. In an interview with the author (March 4, 2020), director of the Health Sector Models Branch of OMHLTC, Sherif Kaldas, confirmed the prioritization of access in the rural context: “We decided from a policy perspective . . . efficiency means little in this setting. It’s access. Are [rural residents] getting equitable access to [the level of hospital care that one associates with] large, urban centers?” In 2012, Ontario introduced its Health System Funding Reform, a plan to transition hospital funding from simple global budgets to a Health Based Allocation Model based on patient populations and organizational performance. In doing so, however, the Ministry of Health recognized that small rural hospitals could not sustain the financial instability likely to result, and excluded such hospitals from the reform (Palmer et al. 2018). It must be emphasized that this kind of attention to and accommodation of the special needs of rural hospitals is not an inherent element of single-payer systems. Rather, it represents a hallmark of how single-payer health care originated and evolved in the Canadian context specifically. While their financial condition may be stabilized to some extent, rural hospitals in Canada remain vulnerable. Because tax dollars pay for health care services, minimizing the per-capita cost of care is an important political objective of Canadian health policy. One interviewee referred to this dynamic as the “efficiency agenda.” Rural hospitals in recent years have been largely protected from major restructuring, but the aforementioned cases of Saskatchewan and Ontario in the 1990s demonstrate the very real possibility of facility closures in remote areas under the banner of efficiency. Health workforce shortages also pose serious problems for rural hospitals, many of which struggle to attract and retain an adequate supply of health professionals. These shortages persist in spite of the considerable political attention paid to them by provincial governments (evident in the array of incentive programs available to rural health workers) and in spite of Canada’s single-payer model. Based on the author’s interviews with rural health stakeholders, there is no indication that a single-payer model naturally produces a more equitably distributed health workforce. This must be accomplished instead through the adoption and expansion of separate workforce-specific policies. Health Services PlanningAs the adage goes, he who pays the piper calls the tune. Aside from the obvious benefits of universal coverage for citizens, perhaps the most impactful advantage of single-payer systems is enhanced governmental authority to plan and manage health services. The power of the purse gives the government—in Canada’s case, provincial governments—tremendous leverage over hospitals and other care facilities. In most provinces, hospital governance has been wrested from local communities and consolidated in regional or provincial health authorities. Even in Ontario, where almost all hospitals are private nonprofit entities with “independent” boards of directors, the government has the legislative authority to take over a hospital and appoint a supervisor, effectively replacing the CEO and the board. Hospital administrators are effectively accountable to the provincial government, so much so that many interviewees in this study colloquially referred to Ontario’s hospitals as “public.” Under the Canadian model, provinces are given both the fiscal flexibility and the decision-making power to experiment with new health sector models. Interviewees expressed confidence that Ontario’s Rural Health Hub model would never have come to fruition if not for Canada’s single-payer system. Without the public funding of participating health systems and the legislative authority to overhaul the existing model, the transition would almost certainly have been infeasible. Nevertheless, it must be underscored that the political will to engage in rural-specific health sector innovation is not an inherent derivative of the single-payer model, but arises from a distinct commitment to fulfilling the unique needs of rural communities. In discussing the two-year lifespan of the Rural Health Hubs, interviewees stressed the ephemerality of Ontario’s health policy programs, instigated by ever-shifting policy approaches and disruptive political transitions. Jim Whaley, a former rural health administrator and consultant, described such pilot programs to the author (March 2, 2020) as “good politics,” a way for politicians to “[do] something without really doing a lot.” Canada’s failure to mount a sustained policy effort in the rural health services sector is disappointing to many experts. When asked if Medicare has lived up to its potential given its rural roots, University of Toronto professor Gregory Marchildon remarked to the author (March 4, 2020) that the program has not “lived up to its full promise.” The combination of private and public payers in the United States, on the other hand, brings different, and arguably more intractable, barriers to large-scale rural policy reform. Given the predominance (68.9%) of private insurance coverage, federal and state governments in the U.S. have less latitude to experiment with disruptive rural health sector models (Cohen, Terlizzi, and Martinez 2019). Much of the reform enacted in this space, such as the global budgeting initiative for rural hospitals in Pennsylvania, has been driven by CMS under its management of the Medicare and Medicaid programs. These piecemeal policy initiatives lack the true scale and scope of the systems-level approach needed in rural health care reform today. Similarly, the ACA, which produced important gains in insurance coverage among rural residents with its funding of Medicaid expansion and premium subsidies through the Marketplace, was hampered both by the intransigence of non-expansion states and by the limitations of its own gradualist design (Benitez and Seiber 2018). In urban and rural areas alike, the central mission of the ACA was to expand coverage, not to fundamentally rethink how health care services are financed or organized—a patchwork approach that has yet to yield convincing improvements in the health status of rural Americans. In 2019, HRSA (2019) released a report, entitled “A Guide to Rural Health Care Collaboration and Coordination,” outlining a strategy for rural providers to improve the integration of care through shared resources, common governance, and increased communication. Occasionally, federal agencies release cogent reports like this one, but do so without the authority to implement suggested reforms on a wide scale and without the funds to sustain them. In this way, the government accomplishes little more than adding pages to the existing volume of wistful recommendations for the future of rural health care in the U.S. Intergovernmental RelationsCanada’s version of strong federalism has implications that are often underappreciated, or overlooked entirely, by American admirers of the Canadian health care system. In his study of the impact of federalism on rural health in the U.S. and Canada, Joe Blankenau (2010) found that Canada’s executive federalism has not fostered the level of rural health policy innovation one might expect, largely due to provincial resistance to federal intervention. With the nexus of health policymaking situated at the provincial level, there is notable interprovincial variation in rural health interest (MacLeod et al. 2007). While some provincial governments have been in the vanguard, demonstrating a firm commitment to action on this issue, others have lagged behind (Sibley and Weiner 2011). The aversion of sub-national governments to federal intrusion is evident across both Canada and the United States. In Canada, the provinces “react suspiciously at any hint of federal incursion in the health care services field” (MacLellan 2002: 41). Similarly, the American states want federal funding on their own terms and are willing to oppose, or sometimes ignore, programs featuring strong federal oversight, a conditional relationship perhaps best characterized as “uncooperative federalism” (Bulman-Pozen and Gerken 2009). Canada’s experience with uncooperative federalism has severely limited the federal government’s ability to move the needle on rural health issues, leaving the 13 provinces and territories to independently design and implement their own solutions. The health policy landscape in the U.S. is even more fragmented. In accordance with the marble cake theory of federalism, rural health policy is a federal-state jumble of governmental agencies and programs. Federal action, dominated by CMS and other HHS entities such as HRSA, is characterized by limited influence over health services planning and the mounting of beneficial, but narrow, programs. When it comes to the current strategy of securing universal coverage via state-level reform, this aspiration has been all but dashed by the halting development of Medicaid expansion under the ACA. Meanwhile, the prospect of extensive state-level rural health reform looks equally grim. According to HRSA’s Rural Health Information Hub, only 24 states have published statewide rural health plans, and only six of these states have updated their plans in the past five years (RHIhub n.d.). The Canadian experience under Medicare demonstrates that the political complications of uncooperative federalism do not disappear under a single-payer health system. If subnational governments are granted greater authority, these complications may even be exacerbated. Champions of single-payer reform in the U.S. have coalesced around a concept of Medicare For All that would ostensibly involve federally centralized funding and administration, but, in reality, a closer analogy to Canada’s Medicare program would be something akin to an expanded Medicaid program. And if the Canadian model is any indication, the notion of 50 or more discrete universal insurance programs operating under the distant supervision of the national government requires serious investigation. Political AccountabilityWhereas the mix of public and private payers in the U.S. dilutes citizens’ power to dissent and incite political action (or inaction, in the case of threatened facility closures), in Canada the lead responsibility played by provincial governments serves to concentrate and channel the will of the citizenry. Many interviewees cited citizen protest as a pivotal factor explaining provincial reluctance to close or restructure rural hospitals. The same threat of political fallout that prompted Ontario’s Health Services Restructuring Commission to convert binding directives to unenforceable recommendations has averted the closure of rural hospitals across Canada. Although an enhanced sense of public accountability in Canada may elevate the voices of neglected rural communities, caveats are necessary. The political preferences of citizens may be out of line with what is considered optimal by health services professionals, such as the commitment to uphold high standards of quality, access, and population health while controlling costs. Because citizens generally lack the technical knowledge of experts, allowing popular opinion to drive health care reform is a risky enterprise. While advantageous for the functioning of representative democracy, politicians’ fixation on constituent approval dampens the willingness of provincial governments to flex their muscle and implement creative changes to rural health policy. Scholars of Canadian health policy have noted how a single-payer model can ironically result in patchwork, “whack-a-mole” reform despite centralized control (Grzybowski and Kornelsen 2013: 11). When it comes to rural health, the influence of electoral politics in shaping the policy agenda is evident. In 2018, Ontario’s incoming Conservative government replaced existing policy—namely, LHINs and Rural Health Hubs—with its own initiative, Ontario Health Teams. While some interviewees saw this reboot as constructive, for others it was little more than political retribution, a classic tale of politicians determined to rhetorically paint over the policy initiatives of their predecessors. In light of such stories, American proponents of a single-payer system who suggest that a Canadian model can, in and of itself, override political dysfunction to facilitate a stable and sustainable rural health policy agenda may be sadly mistaken. Unfortunate ParallelsDespite dramatically different health systems, the U.S. and Canada have a fair deal in common when it comes to rural health. First, and most fundamentally, both nations suffer from significant and persistent urban-rural disparities in health status. Second, health policy and medical education tend to be urban-centric. In an interview with the author (March 5, 2020), James Rourke, co-chair of the Rural Road Map Implementation Committee, described the pervasiveness of what Probst and colleagues (2019) called “structural urbanism”: “The big challenge is that the centers of power and policy are urban centers, [run] by people that don’t have the lived experience, the contextual knowledge of being a rural person. So, often the best, well-meaning policies have rural side-effects and are not helpful. That’s a dilemma in Canada and the world over.” Another commonality lies in the fact that most solutions proposed for rural health problems center around health care financing and delivery while ignoring the distinctive demographic and socioeconomic challenges of rural communities. The health care and social welfare programs adopted in both countries have fallen short in addressing these challenges, though Canada’s social welfare policies are more generous than those of the U.S. (Blank and Hanratty 1993). Summarizing the lack of a cohesive political approach to rural health and health care challenges in both Canada and the United States, Blankenau (2010: 22) lamented: “Policy responses to rural health problems are piecemeal and fragmented and there is no real broad-based rural policy to address the sociological forces driving health problems.” Put simply, neither Canada’s publicly funded health care system nor the United States’ market-driven system have succeeded in alleviating rural health penalty to any laudable degree. ConclusionFor American policymakers interested in the adoption of a single-payer model, Canada’s case presents a complex set of patterns and options. While the Canadian example demonstrates the crucial advantages of a single-payer model, it also demonstrates that these advantages remain largely underrealized, susceptible to shifting political currents and fragmented decision-making within and across governmental jurisdictions. Moreover, the advances exhibited in Canadian rural health care under Medicare seem to be derived as much from a basic value commitment to tackling rural health problems as from the structure of Canada’s single-payer model itself. If nothing else, the experience of our northern neighbor makes clear that the successful design and implementation of a national single-payer program in the United States will require a transition from campaign rhetoric to rational, calculated public policy. For one, the clarification of the states’ role under a potential Medicare For All model is imperative, considering the substantial role of provincial governments in the Canadian Medicare program. Second, the many discrepancies between the two Medicare For All bills previously presented to Congress must be resolved. Only the House bill sponsored by Representative Pramila Jayapal (D-WA) (H.R. 1384, 116th Congress 2019) included specific and meaningful provisions to advance the rural health agenda, such as geographically sensitive global budgeting for institutional providers (Sec. 611(b)(2)(G)(ii)) and priority allocation of capital expenditure funding to medically underserved areas (Sec. 614(c)(2)). The Senate bill sponsored by Senator Bernie Sanders (D-VT) (S. 1129, 116th Congress 2019) went no further than mentioning a vague strategy for improving the collection and evaluation of data on geographic health disparities (Sec. 502). Over the past year, the COVID-19 pandemic has placed incredible strain on the already-struggling rural health care system of the U.S. (Healy et al. 2020; Kliff, Silver-Greenberg, and Kulish 2020). Underscoring the immediate need for structural and creative solutions to the rural health crisis, researchers predict that the pandemic will continue to exert additional financial pressure on rural health care facilities, especially hospitals without CAH status (Bai and Anderson 2020). Today more than ever, policymakers and scholars contemplating the possibilities of a single-payer system in the United States would be well-served by digging deeply into the health care experience of our northern neighbor. Their insights will be much in demand if Americans ever find the political will to resolve the ongoing debate over a truly effective and efficient model for national health reform—one that leaves no one, nowhere, behind. AcknowledgementsI am grateful for the mentorship of Dr. David Rochefort throughout the research and writing process and for the financial support provided by the Northeastern University Office of Undergraduate Research and Fellowships. I am also appreciative for the background information and guidance offered by the generous individuals with whom I conducted interviews while in Toronto and Ottawa, including: Michelle Caplan, Senior Advisor, Ontario Hospital Association; Peter Coyte, Professor of Health Economics, Institute of Health Policy, Management and Evaluation, University of Toronto; Emily Follwell, Policy and Research Analyst, HealthCareCAN; Danielle Fréchette, Executive Director, Office of Research, Health Policy and Advocacy, Royal College of Physicians and Surgeons of Canada; Eric Hanna, President & Chief Executive Officer, Arnprior Regional Health; Sherif Kaldas, Director, Health Sectors Models Branch, Ontario Ministry of Health; Gregory Marchildon, Ontario Research Chair in Health Policy and System Design, Institute of Health Policy, Management and Evaluation, University of Toronto; Gary Mitchell, Consultant, Health System Funding Reform, Ontario Hospital Association; Jonathan Mitchell, Vice-President, Research and Policy, HealthCareCAN; Paul Peters, Associate Professor of Health Sciences, Carleton University; James Rourke, Co-Chair, Rural Road Map Implementation Committee and former Dean of Medicine, Memorial University of Newfoundland; Frank Welsh, Director of Policy, Canadian Public Health Association; Jim Whaley, rural health administrator and consultant (retired); and Jim Wright, Chief, Health Policy, Economics, and Research, Ontario Medical Association. ReferencesAAMC (Association of American Medical Colleges). n.d. “Loan Repayment/Forgiveness/Scholarship and Other Programs.” AAMC.org. services.aamc.org/fed_loan_pub/index.cfm?fuseaction=public.welcome (accessed February 21, 2020). Abelson, Reed. 2019. “Hospitals Stand to Lose Billions Under ‘Medicare for All.’” New York Times, April 21. nytimes.com/2019/04/21/health/medicare-for-all-hospitals.html. Abutaleb, Yasmeen. 2019. “Americans Have Questions About Medicare-For-All. Canadians Have Answers.” Washington Post, November 18. washingtonpost.com/health/americans-have-questions-about-medicare-for-all-canadians-have-answers/2019/11/18/7971c78e-d4d6-11e9-9610-fb56c5522e1c_story.html. Advancing Rural Family Medicine: The Canadian Collaborative Taskforce. 2017a. “The Rural Road Map for Action: Directions.” Mississauga, ON: The College of Family Physicians of Canada and Society of Rural Physicians of Canada. cfpc.ca/uploadedFiles/Directories/Committees_List/Rural%20Road%20Map%20Directions%20ENG.pdf. Advancing Rural Family Medicine: The Canadian Collaborative Taskforce. 2017b. “Summit to Improve Health Care Access and Equity for Rural Communities in Canada: Final Report.” Mississauga, ON: The College of Family Physicians of Canada and Society of Rural Physicians of Canada. srpc.ca/resources/Documents/PDFs/ARFM_Summit_Report_ENG_Final_Web.pdf. Allin, Sarah, and David Rudoler. 2017. “International Profiles of Health Care Systems: The Canadian Health Care System.” New York: The Commonwealth Fund. commonwealthfund.org/sites/default/files/documents/___media_files_publications_fund_report_2017_may_mossialos_intl_profiles_v5.pdf (accessed January 23, 2020). Anderson, Timothy J., Daniel M. Saman, Martin S. Lipsky, and M. Nawal Lutfiyya. 2015. “A Cross-Sectional Study on Health Differences between Rural and Non-Rural U.S. Counties Using the County Health Rankings.” BMC Health Services Research 15: 441. doi.org/10.1186/s12913-015-1053-3. Atkins, Graham T., Taeha Kim, and Jeffrey Munson. 2017. “Residence in Rural Areas of the United States and Lung Cancer Mortality. Disease Incidence, Treatment Disparities, and Stage-Specific Survival.” Annals of the American Thoracic Society 14, no. 3: 403–11. doi.org/10.1513/AnnalsATS.201606-469OC. Baer, L. D., T. C. Ricketts, T. R. Konrad, and S. S. Mick. 1998. “Do International Medical Graduates Reduce Rural Physician Shortages?” Medical Care 36, no. 11: 1534–44. doi.org/10.1097/00005650-199811000-00003. Bai, Ge, and Gerard F. Anderson. 2020. "COVID-19 and the Financial Viability of US Rural Hospitals." Health Affairs (blog), July 1. https://www.healthaffairs.org/do/10.1377/hblog20200630.208205/full/. Barry-Jester, Anna Maria. 2017. “The Health Care System Is Leaving the Southern Black Belt Behind.” FiveThirtyEight, June 28. fivethirtyeight.com/features/the-health-care-system-is-leaving-the-southern-black-belt-behind/. Befort, Christie A., Niaman Nazir, and Michael G. Perri. 2012. “Prevalence of Obesity among Adults from Rural and Urban Areas of the United States: Findings from NHANES (2005-2008).” The Journal of Rural Health 28, no. 4: 392–97. doi.org/10.1111/j.1748-0361.2012.00411.x. Benitez, Joseph A., and Eric E. Seiber. 2018. “US Health Care Reform and Rural America: Results From the ACA’s Medicaid Expansions.” The Journal of Rural Health 34, no. 2: 213–22. doi.org/10.1111/jrh.12284. Bennett, Kevin J., Tyrone F. Borders, George M. Holmes, Katy Backes Kozhimannil, and Erika Ziller. 2019. “What Is Rural? Challenges and Implications of Definitions That Inadequately Encompass Rural People and Places.” Health Affairs 38, no. 12: 1985–92. doi.org/10.1377/hlthaff.2019.00910. Blank, Rebecca M., and Maria J. Hanratty. 1993. “Responding to Need: A Comparison of Social Safety Nets in Canada and the United States.” In Small Differences That Matter: Labor Markets and Income Maintenance in Canada and the United States. Chicago: University of Chicago Press. core.ac.uk/download/pdf/6919226.pdf. Blankenau, Joe. 2010. “Comparing Rural Health and Health Care in Canada and the United States: The Influence of Federalism.” Publius 40, no. 2: 332–49. doi.org/10.1093/publius/pjp043. Booker, Brakkton. 2018. “Rural Poverty In America Is ‘An Emergency.’” NPR, May 21. www.npr.org/2018/05/31/615578001/report-rural-poverty-in-america-is-an-emergency. Bulman-Pozen, Jessica, and Heather Gerken. 2009. “Uncooperative Federalism.” Yale Law Journal 118: 1256–1310. yalelawjournal.org/article/uncooperative-federalism. CDC (Centers for Disease Control and Prevention). 2018. “Table 47. No Health Insurance Coverage among Persons under 65, by Selected Characteristics: United States, Selected Years 1984-2017.” CDC.gov. cdc.gov/nchs/data/hus/2018/047.pdf. CIHI (Canadian Institute for Health Information). 2006. “How Healthy Are Rural Canadians? An Assessment of Their Health Status and Health Determinants.” Ottawa: Canadian Institute for Health Information. secure.cihi.ca/free_products/rural_canadians_2006_report_e.pdf. CIHI (Canadian Institute for Health Information). “National Health Expenditure Trends: 1975 to 2019.” Ottawa: Canadian Institute for Health Information. cihi.ca/sites/default/files/document/nhex-trends-narrative-report-2019-en-web.pdf. Clawar, Meagan, Randy Randolph, Kristie Thompson, and George Pink. 2018. “Access to Care: Populations in Counties with No FQHC, RHC, or Acute Care Hospital.” Chapel Hill, NC: NC Rural Health Research Program. shepscenter.unc.edu/wp-content/uploads/dlm_uploads/2018/01/AccesstoPrimaryCare.pdf. CMS (Centers for Medicare & Medicaid Services). 2019. “FQHC PPS.” CMS.gov, November 13. cms.gov/Medicare/Medicare-Fee-for-Service-Payment/FQHCPPS. CMS (Centers for Medicare & Medicaid Services). n.d. “Ambulance Services.” Medicare.gov. medicare.gov/coverage/ambulance-services (accessed February 21, 2020). CMS Innovation Center. n.d. “Pennsylvania Rural Health Model.” CMS.gov. innovation.cms.gov/initiatives/pa-rural-health-model/ (accessed February 21, 2020). Cohen, Robin A., Emily P. Terlizzi, and Michael E. Martinez. 2019. “Health Insurance Coverage: Early Release of Estimates from the National Health Interview Survey, 2018.” Hyattsville, MD: National Center for Health Statistics. cdc.gov/nchs/data/nhis/earlyrelease/insur201905.pdf. Cole, Evan S., Daniel Walker, Arthur Mora, and Mark L. Diana. 2014. “Identifying Hospitals That May Be At Most Financial Risk From Medicaid Disproportionate-Share Hospital Payment Cuts.” Health Affairs 33, no. 11: 2025–33. doi.org/10.1377/hlthaff.2014.0109. Commission on the Future of Health Care in Canada. 2002. “Building on Values: The Future of Health Care in Canada.” Ottawa: Commission on the Future of Health Care in Canada. publications.gc.ca/collections/Collection/CP32-85-2002E.pdf. Cosby, Arthur G., M. Maya McDoom-Echebiri, Wesley James, Hasna Khandekar, Willie Brown, and Heather L. Hanna. 2019. “Growth and Persistence of Place-Based Mortality in the United States: The Rural Mortality Penalty.” American Journal of Public Health 109, no. 1: 155–62. doi.org/10.2105/AJPH.2018.304787. Cosby, Arthur G., Tonya T. Neaves, Ronald E. Cossman, Jeralynn S. Cossman, Wesley L. James, Neal Feierabend, David M. Mirvis, Carol A. Jones, and Tracey Farrigan. 2008. “Preliminary Evidence for an Emerging Nonmetropolitan Mortality Penalty in the United States.” American Journal of Public Health 98, no. 8: 1470–72. doi.org/10.2105/AJPH.2007.123778. Crosby, Richard A., Monica L. Wendel, Robin C. Vanderpool, and Baretta R. Casey. 2012. Rural Populations and Health. San Francisco: Wiley. Daria, Pelech. 2018. “An Analysis of Private-Sector Prices for Physicians’ Services.” Washington, DC: Congressional Budget Office. cbo.gov/system/files/115th-congress-2017-2018/workingpaper/53441-workingpaper.pdf. Doescher, Mark P., Meredith A. Fordyce, Susan M. Skillman, J. Elizabeth Jackson, and Roger A. Rosenblatt. 2009. “Persistent Primary Care Health Professional Shortage Areas (HPSAs) and Health Care Access in Rural America.” Seattle: WWAMI Rural Health Research Center. depts.washington.edu/uwrhrc/uploads/Persistent_HPSAs_PB.pdf. Dranove, David, Craig Garthwaite, and Christopher Ody. 2017. “The Impact of the ACA’s Medicaid Expansion on Hospitals’ Uncompensated Care Burden and the Potential Effects of Repeal.” New York: The Commonwealth Fund. commonwealthfund.org/sites/default/files/documents/___media_files_publications_issue_brief_2017_may_dranove_aca_medicaid_expansion_hospital_uncomp_care_ib.pdf. Draper, Robert. 2019. “How ‘Medicare for All’ Went Mainstream.” The New York Times Magazine, August 27. nytimes.com/2019/08/27/magazine/medicare-for-all-democrats.html. FCC (Federal Communications Commission). 2019. “2019 Broadband Deployment Report.” Washington, DC: Federal Communications Commission. docs.fcc.gov/public/attachments/FCC-19-44A1.pdf. Fenelon, Andrew. 2013. “Geographic Divergence in Mortality in the United States.” Population and Development Review 39, no. 4: 611–34. doi.org/10.1111/j.1728-4457.2013.00630.x. Fierlbeck, Katherine. 2011. Health Care in Canada: A Citizen’s Guide to Policy and Politics. Toronto: University of Toronto Press. Fleet, Richard, Patrick Archambault, Jeff Plant, and Julien Poitras. 2013. “Access to Emergency Care in Rural Canada: Should We Be Concerned?” Canadian Journal of Emergency Medicine 15, no. 4: 191–93. doi.org/10.2310/8000.121008. Flex Monitoring Team. n.d. “The Flex Program.” FlexMonitoring.org flexmonitoring.org/about/the-flex-program/ (accessed March 19, 2020). Folland, Sherman. 2007. “Does ‘Community Social Capital’ Contribute to Population Health?” Social Science & Medicine 64, no. 11: 2342–54. doi.org/10.1016/j.socscimed.2007.03.003. Foutz, Julia, Samantha Artiga, and Rachel Garfield. 2017. “The Role of Medicaid in Rural America.” San Francisco: Kaiser Family Foundation. kff.org/medicaid/issue-brief/the-role-of-medicaid-in-rural-america/. Frakt, Austin B. 2019. “The Rural Hospital Problem.” JAMA 321, no. 23: 2271–72. doi.org/10.1001/jama.2019.7377. Frohlich, Katherine L., Nancy Ross, and Chantelle Richmond. 2006. “Health Disparities in Canada Today: Some Evidence and a Theoretical Framework.” Health Policy 79, no. 2-3: 132–43. doi.org/10.1016/j.healthpol.2005.12.010. “Full Transcript: Democratic Presidential Debates, Night 1.” 2019. New York Times, June 26. nytimes.com/2019/06/26/us/politics/democratic-debate-transcript.html. Gallup. 2020. “Several Issues Tie as Most Important in 2020 Election.” Gallup.com, January 13. news.gallup.com/poll/276932/several-issues-tie-important-2020-election.aspx. Galvani, Alison P., Alyssa S. Parpia, Eric M. Foster, Burton H. Singer, and Meagan C. Fitzpatrick. 2020. “Improving the Prognosis of Health Care in the USA.” The Lancet 395, no. 10223: 524–33. doi.org/10.1016/S0140-6736(19)33019-3. GAO (General Accounting Office). 1991. “Canadian Health Insurance: Lessons for the United States.” HRD-91-90. Washington, DC: General Accounting Office. gao.gov/assets/160/150584.pdf. Germack, Hayley D., Ryan Kandrack, and Grant R. Martsolf. 2019. “When Rural Hospitals Close, the Physician Workforce Goes.” Health Affairs 38, no. 12: 2086–94. doi.org/10.1377/hlthaff.2019.00916. Goldsmith, Jeff, and Jeff Leibach. 2019. “The Potential Impact of a Medicare Public Option on U.S. Rural Hospitals and Communities: A Scenario Analysis.” Chicago: Navigant Consulting. americashealthcarefuture.org/wp-content/uploads/2019/10/Navigant-Rural-Public-Option-FINAL-8.19.pdf. Gong, Gordon, Scott G. Phillips, Catherine Hudson, Catherine Curti, and Billy U. Phillips. 2019. “Higher US Rural Mortality Rates Linked To Socioeconomic Status, Physician Shortages, And Lack Of Health Insurance.” Health Affairs 38, no. 12: 2003–10. doi.org/10.1377/hlthaff.2019.00722. Grogan, Colleen M., and Sunggeun (Ethan) Park. 2017. "The Racial Divide in State Medicaid Expansions." Journal of Health Politics, Policy and Law 42, no. 3: 539-72. doi.org/10.1215/03616878-3802977. Grzybowski, S., and J. Kornelsen. 2013. “Rural Health Services: Finding the Light at the End of the Tunnel.” Healthcare Policy 8, no. 3: 10–16. doi.org/10.12927/hcpol.2013.23207. Gujral, Kritee, and Anirban Basu. 2019. “Impact of Rural and Urban Hospital Closures on Inpatient Mortality.” Working Paper 26182. Cambridge, MA: National Bureau of Economic Research. nber.org/papers/w26182.pdf. Guzman, Gloria, Kirby G. Posey, Alemayehu Bishaw, and Craig Benson. 2018. “Poverty Rates Higher, Median Household Income Lower in Rural Counties Than in Urban Areas.” Census.gov, December 6. census.gov/library/stories/2018/12/differences-in-income-growth-across-united-states-counties.html. Hale, Nathan L., Kevin J. Bennett, and Janice C. Probst. 2010. “Diabetes Care and Outcomes: Disparities across Rural America.” Journal of Community Health 35, no. 4: 365–74. doi.org/10.1007/s10900-010-9259-0. Hart, L. Gary, Michael J. Pirani, and Roger A. Rosenblatt. 1994. “Most Rural Towns Lost Physicians After Their Hospitals Closed.” Rural Development Perspectives 10, no. 1: 17–21. naldc.nal.usda.gov/download/IND20491801/PDF. Healy, Jack, Sabrina Tavernise, Robert Gebeloff, and Weiyi Cai. 2020. "Coronavirus Was Slow to Spread to Rural America. Not Anymore." New York Times, April 8. https://www.nytimes.com/interactive/2020/04/08/us/coronavirus-rural-america-cases.html?searchResultPosition=24. Hirschfield, Jared. 2019. "Soil to Struggle: A Qualitative Study of Health in Alabama's Black Belt." Harvard Health Policy Review https://6fe7d215-3267-4c00-bed8-ab265d198184.filesusr.com/ugd/f2df11_916bdccdc756443f80b6947db34510bd.pdf. Hofferth, Sandra L., and John Iceland. 1998. “Social Capital in Rural and Urban Communities.” Rural Sociology 63, no. 4: 574–98. doi.org/10.1111/j.1549-0831.1998.tb00693.x. Holmes, George M., Rebecca T. Slifkin, Randy K. Randolph, and Stephanie Poley. 2006. “The Effect of Rural Hospital Closures on Community Economic Health.” Health Services Research 41, no. 2: 467–85. doi.org/10.1111/j.1475-6773.2005.00497.x. HRSA (Health Resources and Services Administration). 2019. “A Guide for Rural Health Care Collaboration and Coordination.” Rockville, MD: U.S. Department of Health and Human Services, Health Resources and Services Administration. hrsa.gov/sites/default/files/hrsa/ruralhealth/reports/HRSA-Rural-Collaboration-Guide.pdf. HRSA (Health Resources and Services Administration). n.d. “Health Center Program: Impact and Growth.” HRSA.gov. bphc.hrsa.gov/about/healthcenterprogram/index.html (accessed February 21, 2020). HRSA (Health Resources and Services Administration). n.d. “National Health Service Corps.” HRSA.gov. bhw.hrsa.gov/loans-scholarships/nhsc (accessed February 21, 2020). iVantage. 2016. “Rural Relevance - Vulnerable to Value: A Hospital Strength INDEX Study.” Newton, MA: iVantage Health Analytics. chartis.com/resources/files/INDEX_2016_Rural_Relevance_Study_FINAL_Formatted_02_08_16.pdf. James, A. M. 1999. “Closing Rural Hospitals in Saskatchewan: On the Road to Wellness?” Social Science & Medicine 49, no. 8: 1021–34. doi.org/10.1016/s0277-9536(99)00180-x. Jones, Esyllt W. 2019. Radical Medicine: The International Origins of Socialized Health Care in Canada Winnipeg, MB: ARP Books. Katz, Josh, Kevin Quealy, and Margot Sanger-Katz. 2019. “Would ‘Medicare for All’ Save Billions or Cost Billions?” New York Times, April 10. nytimes.com/interactive/2019/04/10/upshot/medicare-for-all-bernie-sanders-cost-estimates.html, https://www.nytimes.com/interactive/2019/04/10/upshot/medicare-for-all-bernie-sanders-cost-estimates.html. Kaufman, Brystana G., Sharita R. Thomas, Randy K. Randolph, Julie R. Perry, Kristie W. Thompson, George M. Holmes, and George H. Pink. 2016. “The Rising Rate of Rural Hospital Closures.” The Journal of Rural Health 32, no. 1: 35–43. doi.org/10.1111/jrh.12128. Keith, Katie. 2019a. “ACA Update: Risk Adjustment Litigation, DSH Cut Methodology.” Health Affairs. (blog), September 27. healthaffairs.org/do/10.1377/hblog20190927.674250/full/. Keith, Katie. 2019b. “Health Reform on the Campaign Trail.” Health Affairs 38, no. 12: 1966–67. doi.org/10.1377/hlthaff.2019.01558. Keith, Katie. 2019c. “Continued Uncertainty As Fifth Circuit Strikes Mandate, Remands on Rest of ACA.” Health Affairs (blog), December 19. healthaffairs.org/do/10.1377/hblog20191219.863104/full/. KFF (Kaiser Family Foundation). 2018. “Medicaid Benefits: Non-Emergency Medical Transportation Services.” KFF.org. kff.org/medicaid/state-indicator/non-emergency-medical-transportation-services/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D. Kliff, Sarah, Jessica Silver-Greenberg, and Nicholas Kulish. 2020. "Closed Hospitals Leave Rural Patients 'Stranded' as Coronavirus Spreads." New York Times, April 26. https://www.nytimes.com/2020/04/26/us/hospital-closures-west-virginia-ohio.html?searchResultPosition=18. Kozhimannil, Katy B., Carrie Henning-Smith. 2018. "Racism and Health in Rural America." Journal of Health Care for the Poor and Underserved 29, no. 1: 35-43. doi.org/10.1353/hpu.2018.0004. Kozhimannil, Katy B., Julia D. Interrante, Carrie Henning-Smith, and Lindsay K. Admon. 2019. “Rural-Urban Differences in Severe Maternal Morbidity and Mortality in the US, 2007-15.” Health Affairs 38, no. 12: 2077–85. doi.org/10.1377/hlthaff.2019.00805. Li, Pengxiang, John E. Schneider, and Marcia M. Ward. 2009. “Converting to Critical Access Status: How Does It Affect Rural Hospitals’ Financial Performance?” Inquiry: A Journal of Medical Care Organization, Provision and Financing 46, no. 1: 46–57. doi.org/10.5034/inquiryjrnl_46.01.46. Lindrooth, Richard C., Marcelo C. Perraillon, Rose Y. Hardy, and Gregory J. Tung. 2018. “Understanding The Relationship Between Medicaid Expansions And Hospital Closures.” Health Affairs 37, no. 1: 111–20. doi.org/10.1377/hlthaff.2017.0976. Lopes, Lunna, Liz Hamel, Audrey Kearney, and Mollyann Brodie. 2020. "KFF Health Tracking Poll - January 2020: Medicare-for-all, Public Option, Health Care Legislation And Court Actions." KFF.org, January 30. https://www.kff.org/health-reform/poll-finding/kff-health-tracking-poll-january-2020/. Luthi, Susannah. 2019. “Rural Hospitals Take Spotlight in Coverage Expansion Debate.” Modern Healthcare, August 7. modernhealthcare.com/payment/rural-hospitals-take-spotlight-coverage-expansion-debate. Luthra, Shefali. 2019. “Delaney’s Debate Claim That ‘Medicare For All’ Will Shutter Hospitals Goes Overboard.” Kaiser Health News, June 27. khn.org/news/delaneys-debate-claim-that-medicare-for-all-will-shutter-hospitals-goes-overboard/. MacLellan, Keith. 2002. “A Primer on Rural Medical Politics: 3. Action in Ottawa.” Canadian Journal of Rural Medicine. 7, no. 1: 41. search.proquest.com/openview/b45adb5ceb0080d676adbf576c37cbc6/1?pq-origsite=gscholar&cbl=45825. MacLeod, Martha, James A. Dosman, Judith Kulig, and Jennifer Medves. 2007. “The Development of the Canadian Rural Health Research Society: Creating Capacity Through Connection.” Rural and Remote Health 7: 622. rrh.org.au/journal/article/622. MACPAC (Medicaid and CHIP Payment and Access Commission). 2017. “Medicaid Payment Policy for Federally Qualified Health Centers.” Washington, DC: Medicaid and CHIP Payment and Access Commission. macpac.gov/wp-content/uploads/2017/12/Medicaid-Payment-Policy-for-Federally-Qualified-Health-Centers.pdf. MACPAC (Medicaid and CHIP Payment and Access Commission). 2018. “Rural Hospitals and Medicaid Payment Policy.” Washington, DC: Medicaid and CHIP Payment and Access Commission. macpac.gov/wp-content/uploads/2018/08/Rural-Hospitals-and-Medicaid-Payment-Policy.pdf. Mandich, Anne M., and Jeffrey H. Dorfman. 2017. “The Wage and Job Impacts of Hospitals on Local Labor Markets.” Economic Development Quarterly 31, no. 2: 139–48. doi.org/10.1177%2F0891242417691609. Martin, Danielle, Ashley P. Miller, Amélie Quesnel-Vallée, Nadine R. Caron, Bilkis Vissandjée, and Gregory P. Marchildon. 2018. “Canada’s Universal Health-Care System: Achieving Its Potential.” The Lancet 391, no. 10131: 1718–35. doi.org/10.1016/S0140-6736(18)30181-8. Matthews, Kevin A., Janet B. Croft, Yong Liu, Hua Lu, Dafna Kanny, Anne G. Wheaton, Timothy J. Cunningham, et al. 2017. “Health-Related Behaviors by Urban-Rural County Classification -- United States, 2013.” Morbidity and Mortality Weekly Report 66, no. 5: 1–8. cdc.gov/mmwr/volumes/66/ss/ss6605a1.htm. Meit, Michael, Alana Knudson, Tess Gilbert, Amanda Tzy-Chyi Yu, Erin Tanenbaum, Elizabeth Ormson, Shannon TenBroeck, Alycia Bayne, Shena Popat, and NORC Walsh Center for Rural Health Analysis. 2014. “The 2014 Update of the Rural-Urban Chartbook.” Chicago, IL & Grand Forks, ND: Rural Health Reform Policy Research Center. ruralhealth.und.edu/projects/health-reform-policy-research-center/pdf/2014-rural-urban-chartbook-update.pdf. Multi-Sector Rural Health Hub Advisory Committee. 2015. “Rural Health Hubs Framework for Ontario.” Toronto: Ontario Hospital Association and Ontario Medical Association. oha.com/Documents/Rural%20Health%20Hub%20Framework%20Ontario.pdf. Nasser, Abdullah, and Nancy Chen. 2014. “Telehealth in Rural Canada.” University of Western Ontario Medical Journal 83, no. 1: 49–50. uwomj.com/wp-content/uploads/2014/10/v82no1_16.pdf. Neuhausen, Katherine, Anna C. Davis, Jack Needleman, Robert H. Brook, David Zingmond, and Dylan H. Roby. 2014. “Disproportionate-Share Hospital Payment Reductions May Threaten The Financial Stability of Safety-Net Hospitals.” Health Affairs 33, no. 6: 988–96. doi.org/10.1377/hlthaff.2013.1222. North Carolina Rural Health Research Program. n.d. "179 Rural Hospital Closures: January 2005 - Present (135 since 2010)." ShepsCenter.UNC.edu. https://www.shepscenter.unc.edu/programs-projects/rural-health/rural-hospital-closures/ (accessed February 4, 2021). Oberlander, Jonathan. 2019. "Lessons from the Long and Winding Road to Medicare for All." American Journal of Public Health 109, no. 11: 1497-1500. doi.org/10.2105/AJPH.2019.305295. O’Dowd, Peter. 2019. “Rural Hospitals Say ‘Medicare For All’ Would End Up ‘Closing Our Doors.’” Boston: 90.0 WBUR. wbur.org/hereandnow/2019/08/16/rural-hospitals-medicare-for-all-health-care. Office of the Premier. 2016. “Ontario Launching Pilot Project for Rural Health Hubs.” Government of Ontario, August 7. news.ontario.ca/opo/en/2016/08/ontario-launching-pilot-project-for-rural-health-hubs.html. O’Gorman, Laurel D., John C. Hogenbirk, and Wayne Warry. 2016. “Clinical Telemedicine Utilization in Ontario over the Ontario Telemedicine Network.” Telemedicine Journal and E-Health 22, no. 6: 473–79. doi.org/10.1089/tmj.2015.0166. OMHLTC (Ontario Ministry of Health and Long-Term Care). 1998. “The Rural and Northern Health Care Framework.” Toronto: Ontario Ministry of Health and Long-Term Care. health.gov.on.ca/en/common/ministry/publications/reports/rural/ruralca.aspx. Osgood, Mary H. 1977. “Rural and Urban Attitudes toward Welfare.” Social Work 22, no. 1: 41–47. doi.org/10.1093/sw/22.1.41. Ostry, Aleck. 2012. “The Foundations of National Public Hospital Insurance.” In Making Medicare: New Perspectives on the History of Medicare in Canada, edited by Gregory P. Marchildon, 21-40. Toronto: University of Toronto Press. Palmer, Karen S., Adalsteinn D. Brown, Jenna M. Evans, Husayn Marani, Kirstie K. Russell, Danielle Martin, and Noah M. Ivers. 2018. “Qualitative Analysis of the Dynamics of Policy Design and Implementation in Hospital Funding Reform.” PloS One 13, no. 1: e0191996. doi.org/10.1371/journal.pone.0191996. Parks, S.E., R.A. Housemann, and R.C. Brownson. 2003. “Differential Correlates of Physical Activity in Urban and Rural Adults of Various Socioeconomic Backgrounds in the United States.” Journal of Epidemiology and Community Health 57, no. 1: 29-35. doi.org/10.1136/jech.57.1.29. Petterson, Stephen M., Robert L. Phillips, Andrew W. Bazemore, and Gerald T. Koinis. 2013. “Unequal Distribution of the U.S. Primary Care Workforce.” American Family Physician 87, no. 11. aafp.org/afp/2013/0601/od1.pdf. PHAC (Public Health Agency of Canada). 2018. “Key Health Inequalities in Canada: A National Portrait.” Ottawa: Public Health Agency of Canada. canada.ca/content/dam/phac-aspc/documents/services/publications/science-research/key-health-inequalities-canada-national-portrait-executive-summary/key_health_inequalities_full_report-eng.pdf. Probst, Janice, Jan Marie Eberth, and Elizabeth Crouch. 2019. “Structural Urbanism Contributes To Poorer Health Outcomes For Rural America.” Health Affairs 38, no. 12: 1976–84. doi.org/10.1377/hlthaff.2019.00914. Rechel, Bernd, Aleksandar Džakula, Antonio Duran, Giovanni Fattore, Nigel Edwards, Michel Grignon, Marion Haas, et al. 2016. “Hospitals in Rural or Remote Areas: An Exploratory Review of Policies in 8 High-Income Countries.” Health Policy 120, no. 7: 758-69. doi.org/10.1016/j.healthpol.2016.05.011. Reis, Jared P., Heather R. Bowles, Barbara E. Ainsworth, Katrina D. Dubose, Sharon Smith, and James N. Laditka. 2004. “Nonoccupational Physical Activity by Degree of Urbanization and U.S. Geographic Region.” Medicine and Science in Sports and Exercise 36, no. 12: 2093–98. doi.org/10.1249/01.mss.0000147589.98744.85. RHIhub (Rural Health Information Hub). n.d. “State Rural Health Plans.” Rural Health Information Hub. ruralhealthinfo.org/resources/lists/rural-health-plan (accessed April 10, 2020). Ricketts, T. C. 2000. “The Changing Nature of Rural Health Care.” Annual Review of Public Health 21: 639–57. doi.org/10.1146/annurev.publhealth.21.1.639. Ricketts, Thomas C. 2005. “Workforce Issues in Rural Areas: A Focus on Policy Equity.” American Journal of Public Health 95, no. 1: 42–48. doi.org/10.2105/AJPH.2004.047597. Rochefort, David. 2020. “Making Single-Payer Reform Work for Behavioral Health Care: Lessons from Canada and the United States.” International Journal of Health Services 50, no. 3: 334-49. doi.org/10.1177/0020731420906746. Rochefort, David A., and Kevin P. Donnelly. 2008. “The Changing Influence of the Canadian Single-Payer Model in America’s National Healthcare Debate.” Harvard Health Policy Review 9, no. 1: 132–48. hhpronline.org/past-print-issues/2008. Rosenblatt, R. A., and L. G. Hart. 2000. “Physicians and Rural America.” The Western Journal of Medicine 173, no. 5: 348–51. doi.org/10.1136/ewjm.173.5.348. Rossen, Lauren M., Holly Hedegaard, Diba Khan, and Margaret Warner. 2018. “County-Level Trends in Suicide Rates in the U.S., 2005-2015.” American Journal of Preventive Medicine 55, no. 1: 72–79. doi.org/10.1016/j.amepre.2018.03.020. Seidman, Laurence. 2014. “Medicare for All: An Economist’s Case.” Challenge 56, no. 1: 88–115. doi.org/10.2753/0577-5132560105. Sharkey, Joseph R., Cassandra M. Johnson, and Wesley R. Dean. 2011. “Less-Healthy Eating Behaviors Have a Greater Association with a High Level of Sugar-Sweetened Beverage Consumption among Rural Adults than among Urban Adults.” Food & Nutrition Research 55. doi.org/10.3402/fnr.v55i0.5819. Sibley, Lyn M., and Jonathan P. Weiner. 2011. “An Evaluation of Access to Health Care Services along the Rural-Urban Continuum in Canada.” BMC Health Services Research 11, no. 1: 20. doi.org/10.1186/1472-6963-11-20. Sinclair, Duncan G., Mark Rochon, and Peggy Leatt. 2005. Riding the Third Rail: The Story of Ontario’s Health Services Restructuring Commission, 1996-2000. Montréal: Institute for Research on Public Policy. Singh, Avinainder, Nona M. Jiang, Michael Blaha, Ron Blankstein, and Khurram Nasir. 2019. “Abstract 135: Urban-Rural Differences in Coronary Heart Disease Mortality in the United States in 2010-2015.” Circulation: Cardiovascular Quality and Outcomes 12, no. Suppl_1: A135–A135. doi.org/10.1161/hcq.12.suppl_1.135. Singh, Gopal K., and Mohammad Siahpush. 2002. “Increasing Rural-Urban Gradients in US Suicide Mortality, 1970-1997.” American Journal of Public Health 92, no. 7: 1161–67. doi.org/10.2105/ajph.92.7.1161. Singh, Gopal K., and Mohammad Siahpush. 2014a. “Widening Rural-Urban Disparities in Life Expectancy, U.S., 1969-2009.” American Journal of Preventive Medicine 46, no. 2: e19-29. doi.org/10.1016/j.amepre.2013.10.017. Singh, Gopal K., and Mohammad Siahpush. 2014b. “Widening Rural-Urban Disparities in All-Cause Mortality and Mortality from Major Causes of Death in the USA, 1969-2009.” Journal of Urban Health 91, no. 2: 272–92. doi.org/10.1007/s11524-013-9847-2. Spleen, Angela M., Eugene J. Lengerich, Fabian T. Camacho, and Robin C. Vanderpool. 2014. “Health Care Avoidance Among Rural Populations: Results from a Nationally Representative Survey.” The Journal of Rural Health 30, no. 1: 79–88. doi.org/10.1111/jrh.12032. Stein, Jeff. 2019. “Here Are the Democrats’ Three Key Disputes about Medicare-for-All.” Washington Post, July 31. washingtonpost.com/politics/here-are-the-democrats-three-key-disputes-about-medicare-for-all/2019/07/31/97c18196-b278-11e9-8f6c-7828e68cb15f_story.html. Subedi, Rajendra, T. Lawson Greenberg, and Shirin Roshanafshar. 2019. “Does Geography Matter in Mortality? An Analysis of Potentially Avoidable Mortality By Remoteness Index in Canada.” Health Reports 30, no. 5: 3–15. www150.statcan.gc.ca/n1/en/pub/82-003-x/2019005/article/00001-eng.pdf?st=eo3AQXY5. Syed, Samina T., Ben S. Gerber, and Lisa K. Sharp. 2013. “Traveling towards Disease: Transportation Barriers to Health Care Access.” Journal of Community Health 38, no. 5: 976–93. doi.org/10.1007/s10900-013-9681-1. Symens Smith, Amy, and Edward Trevelyan. 2019. “The Older Population in Rural America: 2012-2016.” ACS-41. Washington, DC: United States Census Bureau. census.gov/content/dam/Census/library/publications/2019/acs/acs-41.pdf. Tarlo, Shira. 2019. “Would Medicare for All Really Force Hospitals to Shutter? The Devil Is in the Details.” Salon, July 28. salon.com/2019/07/28/would-medicare-for-all-really-force-hospitals-to-shutter-the-devil-is-in-the-details/. USDA (United States Department of Agriculture). 2017. “Rural Education At A Glance, 2017 Edition.” Economic Information Bulletin 171. Washington, DC: United States Department of Agriculture, Economic Research Service. ers.usda.gov/webdocs/publications/83078/eib-171.pdf?v=0. USDA (United States Department of Agriculture). 2018. “Rural America At A Glance: 2018 Edition.” Economic Information Bulletin 200. Washington, DC: United States Department of Agriculture, Economic Research Service. ers.usda.gov/webdocs/publications/90556/eib-200.pdf?v=5899.2. Waddell, Kerry, Eilish M. Scallan, and Michael G. Wilson. 2018. “Understanding the Use of and Compensation for Virtual-Care Services in Primary Care.” Hamilton, ON: McMaster Health Forum. mcmasterforum.org/docs/default-source/product-documents/rapid-responses/understanding-the-use-of-and-compensation-for-virtual-care-services-in-primary-care.pdf?sfvrsn=2. Wagnerman, Karina, Joan Alker, Jack Hoadley, and Mark Holmes. 2017. “Medicaid in Small Towns and Rural America: A Lifeline for Children, Families, and Communities.” Washington, DC & Chapel Hill, NC: Georgetown University Center for Children and Families and the North Carolina Rural Health Research Program. ccf.georgetown.edu/wp-content/uploads/2017/06/Rural-health-final.pdf. Whaley, Jim. 2020. “A Longitudinal Review of Rural Health Policy in Ontario.” Healthcare Management Forum 33, no. 2: 53–56. doi.org/10.1177/0840470419886617. Whitacre, Brian E., Denna Wheeler, and Chad Landgraf. 2017. “What Can the National Broadband Map Tell Us About the Health Care Connectivity Gap?” The Journal of Rural Health 33, no. 3: 284–89. doi.org/10.1111/jrh.12177. Wilson, C. Ruth, James Rourke, Ivy Oandasan, and Carmela Bosco. 2020. “Progress Made on Access to Rural Healthcare in Canada.” Canadian Journal of Rural Medicine 25, no. 1: 14–19. doi.org/10.4103/CJRM.CJRM_84_19. Wishner, Jane, Patricia Solleveld, Robin Rudowitz, Julia Paradise, and Larisa Antonisse. 2016. “A Look at Rural Hospital Closures and Implications for Access to Care: Three Case Studies.” San Francisco: Kaiser Family Foundation, The Kaiser Commission on Medicaid and the Uninsured. files.kff.org/attachment/issue-brief-a-look-at-rural-hospital-closures-and-implications-for-access-to-care. Woolhandler, Steffie, David U. Himmelstein, Marcia Angell, Quentin D. Young, and Physicians’ Working Group for Single-Payer National Health Insurance. 2003. “Proposal of the Physicians’ Working Group for Single-Payer National Health Insurance.” JAMA 290, no. 6: 798–805. doi.org/10.1001/jama.290.6.798. Yaemsiri, Sirin, Johanna M. Alfier, Ernest Moy, Lauren M. Rossen, Brigham Bastian, Jane Bolin, Alva O. Ferdinand, Timothy Callaghan, and Melonie Heron. 2019. “Healthy People 2020: Rural Areas Lag in Achieving Targets for Major Causes of Death.” Health Affairs 38, no. 12: 2027–31. doi.org/10.1377/hlthaff.2019.00915. Yang, Tony. 2016. “Telehealth Parity Laws.” Health Policy Brief. Health Affairs, August 15. doi.org/10.1377/hpb20160815.244795. Zuckerman, Stephen, Laura Skopec, and Marni Epstein. 2017. “Medicaid Physician Fees After the ACA Primary Care Fee Bump.” Washington, DC: The Urban Institute. urban.org/sites/default/files/publication/88836/2001180-medicaid-physician-fees-after-the-aca-primary-care-fee-bump_0.pdf. 
From the Inquiries Journal Blog   Related ReadingMonthly Newsletter SignupThe newsletter highlights recent selections from the journal and useful tips from our blog. Suggested Reading from Inquiries Journal
Inquiries Journal provides undergraduate and graduate students around the world a platform for the wide dissemination of academic work over a range of core disciplines. Representing the work of students from hundreds of institutions around the globe, Inquiries Journal's large database of academic articles is completely free. Learn more | Blog | Submit Follow IJ
Latest in Political Science |