Featured Article:Maternal Mortality in Nepal: Addressing the Issue
By
2012, Vol. 4 No. 10 | pg. 1/4 | »
IN THIS ARTICLE
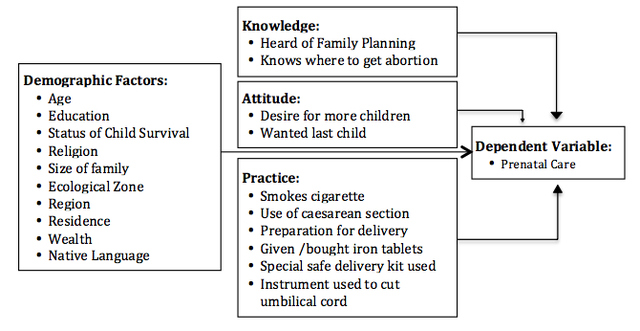
Each year around 358,000 women die because of complications during pregnancy or childbirth and many more encounter serious problems (WHO, 2012). The vast majority of these problems occur in low-income countries, where poverty increases sickness and reduces access to care. These deaths occur within a context of gender-based, economic, political and cultural discrimination and neglect of women’s right to equal status and equitable access to services. Nearly all of these deaths are preventable because the majority of deaths are caused by hemorrhages, sepsis, hypertensive disorders, prolonged or obstructed labor, and unsafe abortions (Rosenfield, & Maine, 1985). Despite its recognition as an important and complex health issue, it was not until 1980s that maternal mortality was added onto the international health agenda as a major public health issue (Suwal, 2008). The patterns of maternal mortality (MM) reveal large levels of inequity between and within countries – 99 % of maternal deaths occur in developing countries and only 1 % of deaths in developed countries (Bhutta et al., 2005). Sub-Saharan Africa leads this death toll, accounting for 50 % of all maternal deaths worldwide (900 deaths per 100,000 live births), and South Asia accounts for another 35 % (500 deaths per 100,000 live births), which is in extreme contrast with the high-income countries (9 deaths per 100,000 live births) (Mills et al., 2009). Despite the commitment of the international community to reduce MM, the magnitude of the problem remains immense. Thus, the goal of the Millennium Development Goals (MDG 5): Reducing MM by three-quarters by the year 2015 has barely been achieved. Over the past 30 years, various community-level interventions have been implemented that include approaches to strengthen healthcare system, to increase awareness about maternal and child health services (MCHs), to provide financial incentives to pregnant women and so on. The UN Population Fund’s (UNFPA) “Global Program to Enhance Reproductive Health Commodity Security” and the World Health Organization’s (WHO) evidence-based guidance in family planning have helped improve access to reproductive health supplies and voluntary use of family planning in more than 70 countries, including in Ethiopia, Laos, Madagascar and Mongolia. Similarly, the UNFPA and the International Confederation for Midwives has been collaborating with individual government of 15 countries in Africa, the Arab States and Latin America to increase the capacity and the number of midwives through formal education, quality training and evaluation. (UN, 2010). Likewise, many countries, like India and Nepal have initiated the Rural Health Mission that conducts community outreach programs on MCH and provides cast incentives to women. Also, in many countries like Nepal, the provision of safe abortion has been legalized as an interventional approach for reducing maternal death (Crane, & Smith, 2006).Maternal Mortality in NepalNepal, a small landlocked country, lies in the central Himalayas, wedged between India and China. With an area of 56,827 square miles and a population of approximately 27 million, Nepal is the world’s 93rd largest country by land mass and the 41st most populous country (ImNepal, 2012). Maternal mortality (MM) is one of the major health issues in Nepal. In 1996, the Nepal Family Health Survey estimated maternal mortality ratio (MMR) to be 539 per 100,000 live births, which was the highest among the South-Asian countries at that time. The Demographic Health Survey (DHS) 2006 showed Nepal’s MMR as 281 per 100,000 live births, a decrease by almost 50% (Suwal, 2008). For this significant progress and commitment towards improving maternity health goal under the MDG-5, Nepal was honored at the 2010 Millennium Development Goals Review Summit. The MMR was lowest amongst women in twenties, with increased risk for those aged under 20 and between 30-34. The figure for those aged over 35 was considerably higher (962 per 100,000 live births). There were also differences between ethnic groups, with higher rates among Muslims, Terai /Madhesi and Dalits (Nepal Monitor, 2010). Pregnancy and delivery-related causes are among the top ten reasons for MM in Nepal. The main direct cause, hemorrhage, has been dramatically reduced, down from 41% in 1998 to 24% in 2006. The decline reflects a reduction in postpartum (from 37% to 19%), rather than antepartum. The contributions of eclampsia, abortion related complications, gastroenteritis and anemia have increased, while those from obstructed labor and puerperal sepsis have more than halved since 1998. Heart disease accounts for 7%. There was an increase in the proportion of pregnancy related deaths occurring in a health facility, to 41%; with 40% occurring at home; and 14% in transit. In 1998 just 21% of deaths occurred in facilities and 67% at home (Nepal Monitor, 2010). Many pregnancies were unwanted; suggesting the pregnancy status of the women may have placed them at greater risk. Of the total MM, 39% occurred during the intrapartum period and up to 48 hours afterwards and 61% in the antepartum and postpartum periods suggesting that interventions should focus more on this period. Over 80% of women who died from maternal causes were emergency admissions in a critical state. MM also caused indirectly by hepatitis, diabetes, malaria, infections, malnutrition, and anemia. The indirect causes, though preventable, contribute to about 24% of all maternal deaths in the world (Weston, 1986). Risk Factors in NepalTraditionally, pregnancy is considered to be natural in Nepal. Thus, regular check-ups are thought to be unnecessary, particularly in rural areas, unless there are complications. One study unveiled that some groups of women in Nepal do not seek prenatal care (PC) because they think infants were more likely to die if they do so while these infants were in the womb (Suwal, 2008). Such norms were found in other developing countries like Egypt, as well. Women’s as well as their families’ (especially husbands and mother-in-laws) perception about MHS were averting women from receiving PC, thus, increasing risk of maternal mortality. However, the proportion of mothers who receive PC from skilled birth attendants (SBAs), increased from 24% in 1996 to 44% in 2006. This might be one of the factors for reduced maternal mortality in recent years (Puri et al., 2008). Also, life-style and different cultural practices of various ethnic groups in Nepal showed a remarkable impact on MM. For example, Mongoloid women’s almost 50% lower probability of dying of maternal causes compared to orthodox Brahmin and Chettri women supports the “women’s empowerment” theory strongly. It is not only the high status and autonomy of Mongoloid women but also their late age at marriage, the affection and respect their spouses and family members give them affect their mortality related to reproduction (Suwal, 2008). Likewise, factors such as early marriages, frequent births, and high parity create health hazards to women. In many rural areas of Nepal, early marriage is customary. Sending young girls off in marriage is a big relief in some cultures such as in the Terai plains of Nepal where dowry and tilak are compulsory and the tilak amount goes higher as unmarried girls grow older. Marrying early, consequently, conceiving early is taking more lives of women than Nepalese realize. Also, frequent births entail repeated life-threatening processes. Moreover, some reports show that 50% of all maternal deaths in Nepal (where abortion was illegal until September 2002) were due to induced abortion (Suwal, 2008). Unsafe, unhygienic and sometimes fatal natures of practices conducted by traditional birth attendants were the reasons for maternal deaths in such cases (Thapa et al., 1994). Other attributed factors for high MM are the 'three delays' - delay in taking the decision to seek medical assistance, delay in accessing appropriate care and delay in receiving care at health centers. Delay in seeking help due to cultural beliefs, problems of finance, transport, and decision-making has been reported by a number of studies in Nepal (Suwal, 2008). Many Nepalese people, especially in rural areas believe that the complication is created by an evil eye and thus seek help from traditional healers (Shamans) before seeking medical help. Also, many women do not seek prenatal care because they are unaware of its benefits (Ministry of Health, 1998). Furthermore, many district hospitals are unable to cope with obstetric emergencies. Among other problems, drugs are not always readily available in the pharmacy and if available, the poor families are unable to buy. In addition, the health care staffs in the rural health posts are often reported as being unreliable, hostile towards local patients, and absent from the care centers; the major probable causes of not seeking medical care by rural women even when medical care was available (Suwal, 2008). Furthermore, most women in rural areas of Nepal are forced to perform daily household chores and fieldwork that demands physical strength. Also, sanitation, a factor that affects MM, is extremely poor in home, where almost all the deliveries take place (Ministry of Health, 1996/1997). The 2006 Nepal Demographic Health Survey (NDHS) revealed that 82% of all women give birth at home and a skilled professional attends only 18% of those births. This is a result of a range of socio-economic and cultural barriers to service use. As a result of the high proportion of home deliveries, low use of professional care at birth, low utilization of PC and inadequate availability of health services, many Nepali women continue to suffer from pregnancy related complications. For example, only 44% of women who gave birth received at least one prenatal care contact with a health professional (Puri et al., 2008). In rural areas, the rate was even lower, at 38%. Only 19% of women delivered their babies with the assistance of a SBA (doctor, nurse or midwife) and 18% at a health facility. The percentage of births assisted by relatives and others has declined very little over the 10-year period before the survey (NDHS, 2006). Preliminary AnalysisIn Nepal, where a woman dies every four hours due to pregnancy-related causes, use of prenatal care (PC) has been minimal. According to the NDHS 2006, more than 80% of deliveries occurred at home in the absence of SBAa and only 29% of total women made the recommended four prenatal visits (NDHS, 2006). Various scientific studies have shown that PC, which helps women to identify complication and potential risks and gives direction to plan for safe delivery, is a significant component of maternal health. For example, the most important evidence includes the distribution of iron, foliate and malaria prophylaxis can help to improve the nutritional status of women making them better able to withstand hemorrhage and prolonged labor and improve chronic anemia (Suwal, 2008). Also, blood pressure monitoring can prevent deaths from toxemia. Significance of PC visit can go beyond pregnancy period because; women who seek PC generally also tend to seek assistance from a health professional during childbirth. Hence PC utilization is an important determinant of use of safe delivery care, which in turn reduces MM (Prata et al., 2010). Figure 1 - A framework summarizing the factors associated with maternal mortality
This study presents findings from the analyses of Nepal Demographics and Health Survey 2006 (NDHS) data. For this study, we used utilization of prenatal care (PC) by women as a key factor in maternal mortality in Nepal. Respondents were asked whether they had seen anyone for PC during the pregnancy preceding each live birth in the last five years. From the database, the variable “PC,” a dichotomous variable with responses “No: did not receive PC” and “Yes: received PC” was used as a dependent variable. Out of 4182 mothers, 1161 mothers (27.8%), did not seek PC whereas the rest, 3021 mother (72.2%) sought some kind of PC. Associations between PC status (received care vs. no care) and four major groups of independent variables (demographic factors, knowledge, attitude and practice) were investigated in the analysis. Demographics characteristics included ten variables: mother’s age, type of place of residence type, ecological zone, regions, mother’s highest educational attainment, number of household members, religion, wealth index, native language of mother and survival status of previous child. According to Independent samples t-test, there was no significant difference in the mean number of household members between the two PC status groups (t(4182)=.307, p=.78). However, we observed a significant difference in the mean age of women between the two PC status group (χ2 = 226.207, p = <.001). Majority of the women in the age group 20-34 years and younger age group received PC, the highest percentage (82.9%) being in the 15-19 years of group. In contrast, majority of women belonging to 35-39 age group or higher did not receive PC, the highest being 67.9%) being in the 45-49 age group.Continued on Next Page » 
From the Inquiries Journal Blog   Monthly Newsletter SignupThe newsletter highlights recent selections from the journal and useful tips from our blog. Suggested Reading from Inquiries Journal
Inquiries Journal provides undergraduate and graduate students around the world a platform for the wide dissemination of academic work over a range of core disciplines. Representing the work of students from hundreds of institutions around the globe, Inquiries Journal's large database of academic articles is completely free. Learn more | Blog | Submit Follow IJ
Latest in Health Science |