HIV-Positive Youth Empowerment in Swaziland: An Evaluation of the Social Stigma Surrounding HIV
2014, Vol. 6 No. 06 | pg. 1/2 | »
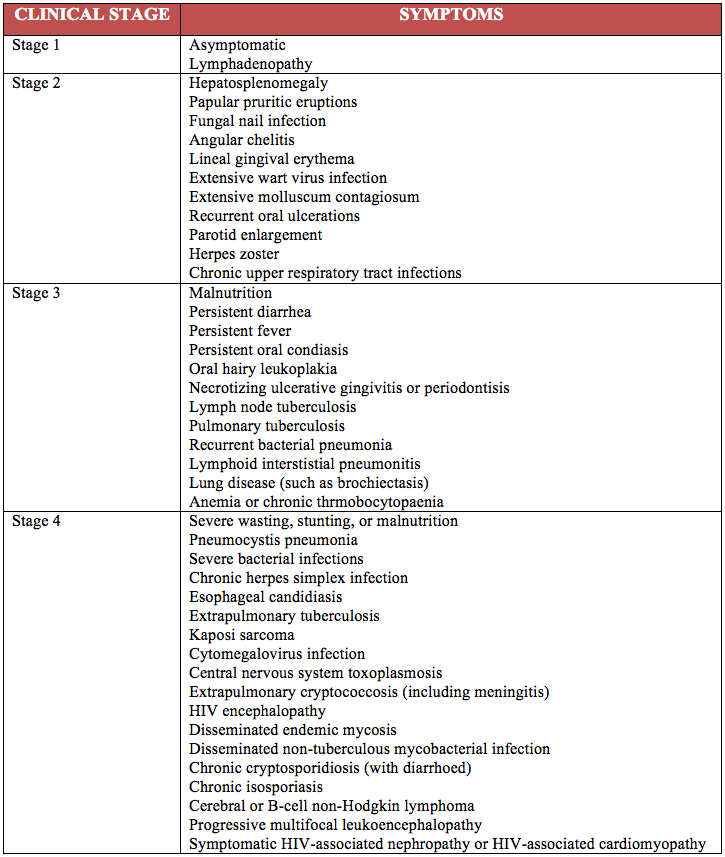
UNAIDS reports the antenatal HIV prevalence rate—the prevalence of HIV in unborn children—to be approximately 38% in Swaziland, Africa (UNAIDS 2012), the highest rate in the world (Root 2010). Diagnosed through an HIV antibody test or virological analysis, clinical progression of HIV infection is often divided into four stages based on symptoms observed in children (Table 1) (World Health Organization 2007). Disease progression through the stages into AIDS or death is reduced through antiretroviral medications, which have shown long term reversals in the infection’s effects on plasma molecules such as CD4 cell levels and HIV-1 RNA concentrations over a period of several years. (Grabar et al., 2005) In Swaziland, there are a number of clinics available to provide such antiretroviral medications, including the Baylor International Pediatric AIDS Initiative (BIPAI) clinic in association with the Baylor College of Medicine (www.bipai.org).
A Swazi woman preparing an HIV awareness badge (Avert.org).
{kind=link}
Advertisement
Figure 1: Swaziland population age distribution, 2010 and 2050 (projected). (From International Conference on Population and Development Beyond 2014.)
{kind=link}
However, in conjunction with antiretroviral therapy that is already available in Swaziland and expanding throughout the country, empowerment therapies such as confidence development, psychosocial peer support, and life rehabilitation are vital for optimal personal and communal growth. This is due to the high levels of social stigma that discourage HIV-positive individuals from becoming leaders and contributing to their communities. Stigma, as defined by Goffman (1963) is defined as a “differentness” associated with a group affiliation, in this case HIV-positive status. The purpose of this report is to analyze the current state of HIV in Swaziland in order to better understand the need for empowerment therapy for HIV-positive adolescents within the country. The concept of a novel, three-part pen pal program will be introduced to empower HIV-positive adolescents in Swaziland towards leadership and confidence.
The Current State of HIV in Swaziland
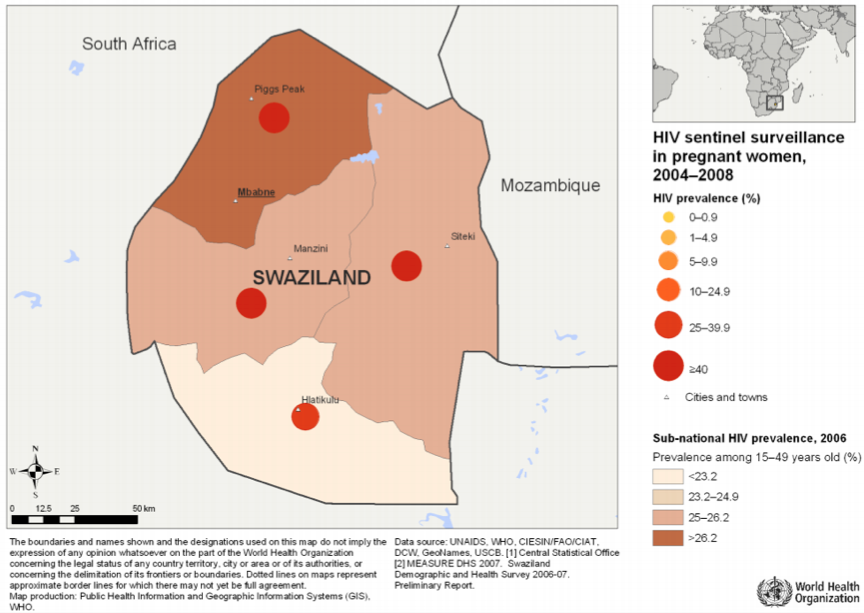
Swaziland is a sub-Saharan African country with a total population of just over 1,000,000 individuals (Figure 1), with a life expectancy of 48 years for men and 47 years for women (International Conference on Population and Development Beyond 2014) and an overall HIV prevalence of 26% for individuals ages 15 to 49 (UNAIDS and NERCHA 2010) (Figure 2). Mother-to-child transmission of HIV is the second most common cause of HIV infection in Swaziland, second only to unprotected heterosexual contact (Whiteside, Hickey, Ngcobo, & Tomlinson 2003). As such, it is not surprising that only 16% of women and men ages 15 to 49 in the country received an HIV test in the past year. This lack of regular testing despite a high HIV prevalence rate in Swaziland, as well as a mere 59.2% of men with multiple partners reporting the use of condoms, has lead to a severe increase in HIV prevalence in pregnant women from only 3.9% in 1992 to a shocking 41.1% in 2010 (UNAIDS 2012). With only 59.2% of adults and children who are HIV-positive receiving antiretroviral therapy, approximately 78,000 children under the age of 18 have been orphaned as a result of HIV/AIDS in Swaziland. (UNAIDS 2014).
Figure 2: HIV prevalence in Swaziland by region among 15-49 year old individuals and in pregnant women. (From World Health Organization 2006-2007.)
{kind=link}
Social Stigma in Africa Necessitates Empowerment Therapy for HIV
High rates of HIV in Swaziland have led to high rates of social stigma. As a result, research studies using surveys and case studies have been recently released to better understand the forms of stigma that exist both in Swaziland and other African countries.
In a study that held focus groups of a total of 111 males and females living with HIV/AIDS from five African countries—Lesotho, Malawi, Swaziland, South Africa, and Tanzania—both physical and verbal abuse were reported, in addition to overall neglect and rejection by the community (Dlamini et al., 2007). With regards to physical abuse, participants in the study reported incidences of family members beating the HIV-positive individuals or their possessions being taken from them and destroyed. HIV-positive individuals also experienced a wide range of verbal violence, including insults and name-calling, specifically directed at either the mortality of those individuals or putting blame on them for contracting the infection. In addition to these forms of abuse, participants in the study also noted instances of familial rejection as well as denial to community resources. Children who were HIV-positive reported being suspended from their schools or even being unable to attend church.
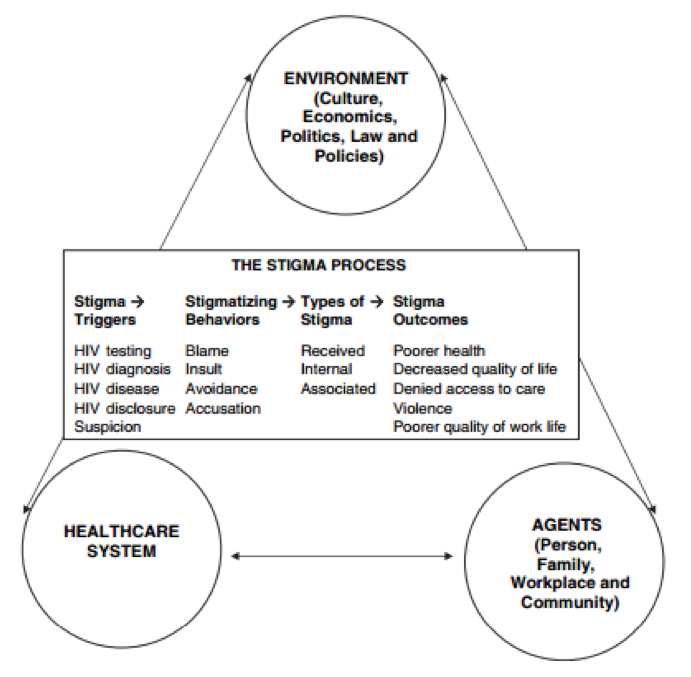
Ultimately, the study identified three sources of abuse of HIV-positive individuals (Dlamini et al., 2007). The first is abuse by family members, who often refuse to assist in doctor’s visits or daily care. The second source of abuse is at the workplace; although no cases of physical abuse at work were reported, verbal abuse is common, despite laws established to omit discrimination of HIV-positive individuals at work. As a result of these sources of abuse, the study reports that HIV-positive individuals fear disclosing their disease status. However, this fear only intensifies the social stigma of HIV/AIDS (Dlamini et al., 2007). From the results of the focus groups, a model of HIV-AIDS stigma was developed (Figure 3).
Figure 3: HIV/AIDS model for social stigma. (From Holzemer et al., 2006.)
Advertisement
{kind=link}
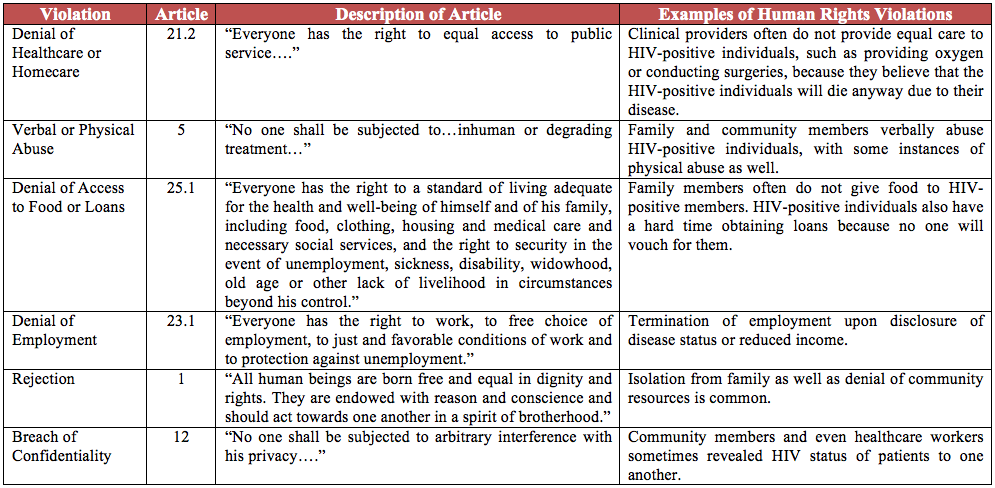
Research has also focused on understanding the human rights violations associated with the social stigma of HIV. Human right violations were analyzed using the African Charter of Human and People’s Rights (African Union 2003). Six violations of basic human rights were described to be in practice within the five African countries, as outlined in greater detail in Table 2: (1) Denial of healthcare or homecare, (2) verbal or physical abuse, (3) denial of access to food or loans, (4) denial of employment, (5) rejection, and (6) breach of confidentiality (Kohi et al., 2006).
Table 2: Various violations of human rights and examples of such violations. (The results of Kohi et al., 2006 were re-organized and modified to present in this tabular format.)
{kind=link}
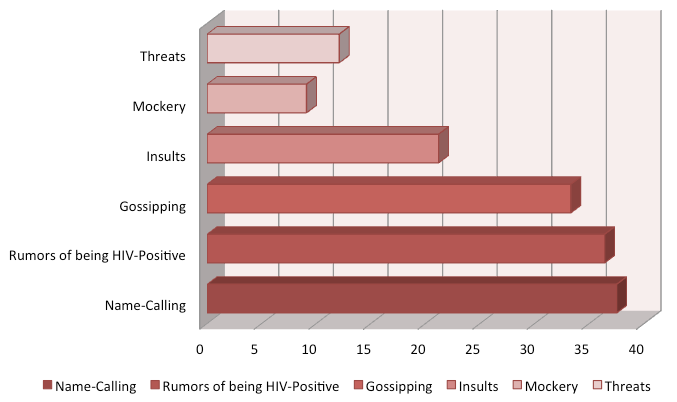
Specifically within Swaziland, questionnaire data of 33 HIV-positive individuals reports a high prevalence of verbal abuse and overall social stigma (Root 2010). Various forms of verbal abuse, such as name calling and spreading of rumors, were reported at high rates, as shown in Figure 4. Social modes of stigma were less prevalent, but HIV-positive individuals reported loss of social networks (18.2%), decreased visits from neighbors (15.1%), being spoken to differently (12.1%), exclusion from events (12.1%), visits by others to mock them, and being viewed as having no future (12.1%), among others. Interestingly enough, several participants in the study claimed that they were prohibited from eating with their families (18.2%), doing household chores (12.1%), and sharing utensils, clothing, and bedding with the rest of the family members (9.1%). This is likely due to a lack of education about the modes of transmission of HIV within Swaziland communities (Root 2010).
Figure 4: Prevalence rates of HIV-related verbal abuse in Swaziland (Root).
{kind=link}
Given the high levels of social stigma present within Swaziland associated with HIV, it is critical to provide empowerment opportunities for HIV-positive adolescents to become confident leaders in their communities despite that stigma. Studies from various countries show that HIV-positive adolescents are also affected by social stigma. For instance, a large-scale study in Haiti found that 32% of caregivers of HIV-positive adolescents reported that those adolescents were discriminated against. Therefore with a lack of child social support, the adolescent considers himself or herself as an orphan, which increases the risk of perceived discrimination (Surkan, et al., 2010). In addition, because HIV-positive individuals, adults and adolescents alike, who experience social stigma are significantly more likely to not adhere to their antiretroviral therapy medications (Martinez et al., 2012), leadership building fosters self-respect, resilience, and confidence.Continued on Next Page »