Guns and Suicidal Thoughts in Adolescence: An Understudied Relationship
2022, Vol. 14 No. 05 | pg. 1/1
Abstract
The prevalent school of thought states that suicidal ideation and suicide planning are not associated with living in households with firearms. Using data from the National Longitudinal Study of Adolescent to Adult Health (Add Health) in the years 1994 and 1995, I use multiple logistic regression models to estimate the effect of the availability of guns on the odds of adolescents in those households experiencing suicidal thoughts. By matching across several key demographic and psychosocial variables, I approximate a randomized treatment assignment. I find evidence that contradicts the prevalent school of thought. The data analysis shows that the presence of guns has a statistically significant “effect” of increasing a respondents’ self-reported odds of having suicidal thoughts, even as I control for key demographic and several other key variables. Viewed in the larger political context these results add additional nuances to the discourse around accessibility of firearms for adolescents since they show that they could negatively impact self-reported psychological health even if all the standard of security are being obliged to.
Introduction
Does gun ownership increase suicidal thoughts in adolescents? In 2019, suicide was the 10th leading cause for death in the US with more than 40.000 people - over 120 a day - taking their own lives. Firearms account for almost half of these deaths (American foundation for suicide prevention). At the same time and at latest since the Sandy Hook shooting in 2012, gun ownership and the access to guns has been a heavily debated topic in US politics. Especially if we compare the US to other industrialized countries we find that adults and also teenagers have comparatively easy access to firearms. Overall, scholarly research in the past has shown that gun ownership is clearly correlated with a higher suicidal rate (Miller, Lipmann, Azrael & Hemenway, 2007). However, although there is seems to be a positive correlation between gun ownership and suicide rates, some studies find that this does not necessarily imply that gun ownership is associated with suicidal thoughts (Ilgen, Zivin, McCammon, & Valenstein, 2008). Using data from the National Longitudinal Study of Adolescent to Adult Health (Add Health) in the years 1994 and 1995, I use multiple logistic regression models to estimate the effect of the availability of guns on the odds of adolescents in those households experiencing suicidal thoughts. By matching across several key demographic and psychosocial variables, I try to approximate a randomized treatment assignment. However, since I am using observational data I refrain from making a casual claim. I find evidence that contradicts the prevalent school of thought. My findings show that the presence of guns has a statistically significant “effect” of increasing a respondents’ self-reported odds of having suicidal thoughts, even as I control for key demographic and several other key variables.
Theory
The relationship between gun ownership and suicide rates has extensively been studied. A World Health Organization Report from 2002, for example, clearly lays out how having “access to the means to kill oneself (most typically guns[…])” is a significant factor in increasing the risk of potential self harm and suicide attempts. This finding is not limited to a certain age group. More specifically, Knopov et al find in their 2019 paper that household gun ownership is positively related to youth suicide rate. This association has been widely replicated and shown in many other, often older, studies (Lester, 1989). However, less established is the relationship between gun ownership and suicidal ideation, meaning thinking about suicide but not necessarily carrying it out. Some research has been done on this and the studies hint at the theory that gun ownership might not necessarily be associated with suicidal ideation (Khazem, et. al.2016). This finding is replicated by another study. According to research done by Miller et al.suicidal ideation and suicide planning are not associated with living in households with firearms (Miller et al, 2009). Additionally, the same study finds that the likelihood to develop anxiety disorders, mood disorders or substance abuse is as high for people living in a home with firearms as for those without it (Miller et al, 2009). Moreover, some research with suicide-survivors shows that many suicide attempts are impulsive (Simon TR, Swann AC, Powell KE, et al, 2001). All this could hint at the following: Firearms could be associated with higher suicide rates because they are used impulsively and very effectively to commit suicide. However, owning firearms might not actually be related to the thoughts that end up leading to the actual suicide attempt but just to a higher fatality rate. My motivation with this analysis is to try and assess the relationship between gun ownership and suicidal ideation among adolescents and see whether my analysis confirms prior results or whether we might find contradicting evidence to the prevalent school of thought.Data
In the following analysis, I make use of the data from the National Longitudinal Study of Adolescent to Adult Health (Add Health). The Add Health data set is compiled of a nationally representative sample of adolescents in grades 7 to 12 from the United States of America. The full dataset was gathered over a period of several decades. However, the data used for the purposes of this analysis was recorded only during the 1994-95 school year.
Advertisement
My analysis deals with the issue of suicidal thoughts among teenagers. I, therefore, use the answer to the question “during the past 12 months, did you ever seriously think about committing suicide?” as a proxy for suicidal ideation. The binary variable for suicidal ideation (“suicide”) differentiates between every respondent that reported having thought at least once or more about committing suicide in the past year (1) and those respondents that reported no serious suicidal thoughts (0). I also filtered out all those respondents which did actually attempted suicide in the past 12 months since in this analysis I am concerned with suicidal ideation but not with actual suicide attempts.1 There could be a systematic differences between the group that actually carried out suicide attempts and the one that did not. For the purpose of this analysis, I will only be concerned with those respondents that reported having suicidal thoughts but did not try to carry them out. As my main explanatory variable for possible suicidal ideation I used the variable “gun” which describes whether a gun was easily available at home of the respondent or not (will be referred to as “gun ownership”). Herefore, I code a binary variable that depicts whether a respondent had easy access to a gun at home (1) or did not have easy access to guns (0). It is important to note here that I am not making a distinction between subjects that owned firemarms themselves and between those where the gun available at home was property of the parents or guardians. Since I am dealing with a sample of adolescents I assume that in general, the firearms were property of the parents (more on this in VI. Discussion).
In line with previous research, I have additionally included a variety of demographic variables in the regression analysis such as the binary variable female (1 - if respondent is a female, 0 if respondent is male), a numeric variable for the age, health situation (poor, fair, good, very good, and excellent, ranging from 0 to 4) and intelligence (moderately below average, slightly below average, about average, slightly above average, moderately above average, extremely above average - ranging from 0 to 5) of the respondent and several categorical variables such as the respondent’s race (white, black, hispanic, asian, american indian or “other”) and religion (no religion, baptist, catholic, jehovah’s witness, jewish-conservative/reformed/orthodox/reconstructionist, islam/moslem/muslim, lutheran, methodist, christian church (Disciples of Christ) or “other”). Additionally I have included two more binary variables which have special importance. The first one is the variable “substance abuse.” To code this variable I used the answer to the question “in the past year, have you attended a drug abuse or alcohol abuse treatment program?.” This binary variable is used as a proxy to differentiate between respondents that engaged in heavy substance abuse (1) and those that did not (0). The last variables that is important to mention codes whether a respondent has received emotional or psychological counseling in the past 12 months (1 if yes, 0 if no). This information is coded in the binary variable “psychological problems” and used as a proxy for possible depression or emotional stress.
As with most large datasets, the Add Health data suffers from missing responses for some of our covariates. Since I cannot make an inference on whether the missingness is random or systematic I impute missing values with the Amelia package in order to avoid a possible bias. I impute data only for the independent variables2 but not for my outcome variable to prevent inducing a relationship between independent and dependent variable by construction. The missingness is very pronounced for the variables race (39.6% of entries missing), health (30%), female (27.5%) and age (27.2%). However, the missingness is less than 2.2% for all other variables, including the dependent and independent variable of interest (gun). Therefore, although missingness is a problem in the Add Health data, I do not believe it to be very severe with regard to the analysis since most of the important variables are left fairly untouched by it. (see Appendix under 6. Missingness for missingness graphs).3
Table 1 below presents a summary statistic of the most important covariates after the imputation has been conducted. The table is meant to give a general overview of the distribution of the numbers in both groups (those that had suicidal thoughts and those that did not). For additional information on the summary statistics please refer to several additional summary statistics tables in the Appendix.
By looking at the data we can see that some covariates like age or female differ between treatment and control group. To solve this imbalance in the data and to approximate the process of random treatment in which the treated and the control populations are, on average, balanced across that set of covariates, I use covariate balancing propensity score (CBPS) weights.[4] Analysis of the data has shown that CBPS matching does, compared to other matching methods like “nearest” or “subclass,” the best job at reducing the imbalance between treatment and control groups.[5] In the case of this data the two groups were fairly similar before CBPS matching was conducted (and after imputation). However, there are a few variables that stand out. The “treatment” group (those with guns) was encompassed of a substantially larger portion of white respondents than the control group (72.1% vs.56.2%). Also, the treatment group was slightly older (15.08 vs.14.83 years) and more predominately male (60% of treatment group are males vs.43% in control group). Aside from this, most important characteristics like intelligence, health, substance abuse and psychological problems were fairly similar even before CBPS matching was conducted. Once matched, all characteristics are very similar across treatment and control groups (data is more balanced). Even “white” (72.1% of treatment group are white vs.71.5% control group), age (15.08 for both), and male composition (58.1% of treatment group are males vs.57.6% in control) are very well matched. Also note, since CBPS matching uses weights we are not loosing sample size, which is another advantage of this procedure.[6]
Methods
To test the theory I constructed four different logistic regression models, ranging from a “basic” model with one explanatory variable (gun), to a full model with a variety of control variables, including such terms as psychological problems or substance abuse. As explained above, our outcome variable is binary (suicidal thoughts: yes (1), no (0)). I used logistic regression because it is ideally suited for binary dependent variables. The outcome can be described as the probability (here: of a respondent having suicidal thoughts) as a function of our explanatory variables (guns available at home). In light of the question I am addressing, this approach is analytically useful since the probability of having suicidal thoughts is limited to a number between 0 and 1 (the chances for a subject to have suicidal thoughts are somewhere between 0% and 100%). Our logit model therefore limits our predictions within the range of 0 and 1, which the OLS model does not allow to do. Additionally, and as mentioned before, CBPS matching was conducted prior to running the regressions to approximate a random treatment (see III. Data).
I conducted several ANOVA tests to compare the four different models and determine which model best balances explanatory power and the complexity of adding more variables to the regression. Running the ANOVA tests shows that the fourth model provided the best trade-off between explanatory power and complexity.7 The equation for model 4 is the following:
Below, in the results section, I will present all four models with their covariates and their respective coefficients. However, the focus of my analysis will lie heavily on model 4 since it has proven to provide the best trade-off between explanatory power and complexity.
Advertisement
Last but not least I want to shortly mention some of the key assumptions of logistic regression and discuss whether they are fulfilled or not. First, binary logistic regression needs the outcome variable to be binary. This is fulfilled since our dependent variable “suicidal ideation” can only take on the values “yes” (1) or “no” (0). Second, this type of regression analysis requires the observations to be independent from each other (similarly to OLS). This seems fulfilled too, since I assume that the different subjects interviewed did not know or communicate with each other. Thirdly, logistic regression requires, again similarly to OLS, small multicollinearity between the covariates. This third assumption is met too.8 All in all, the basic conditions for logistic regression seem to be met.
Results
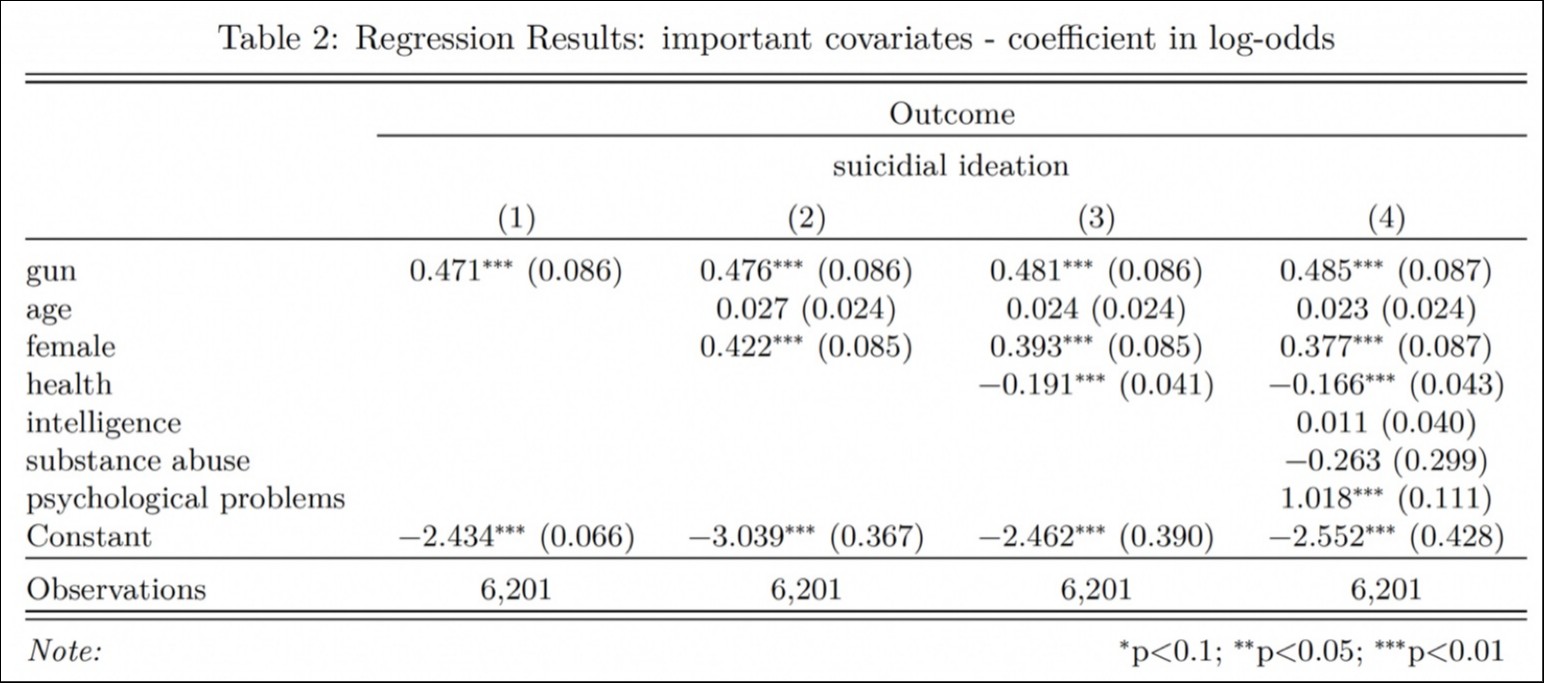
Below I present a table of the relationship between our key explanatory variables and our outcome of interest (using logit regressions for each model). Due to limited space I only included the main variables of interest. The coefficients in the table represent the change in log-odds.9
{kind=link}
I want to repeat that for this analysis I am making use of observational data. Even after using CBPS matching the results I present do not allow any conclusion on causal relationship between gun ownership (“treatment”) and suicidal thoughts. There still exists a possibility of bias and confounding by observable or unaccounted for variables. I, therefore, treat the results as an association and will not use them to make causal claims. As we can see above, I find a statistically significant relationship for my main explanatory variable across all four different models.10 As we can see below, generally, it appears that going from “no gun” to “gun,” all else equal, increases the chances of that adolescent respondent having suicidal thoughts. More specifically, and for our preferred model 4, a one unit move in the main variable of interest (no gun to gun) is associated with a multiplicative increase of 1.624 (or ) in the odds of a respondent having suicidal thoughts, holding all other demographic variables constant. This result is statistically significant at the 1% level (p-value of 2.65e-07).
My results are substantively important since they provide evidence that contradicts the findings that gun ownership is not related to suicidal ideation. According to our results, there seems to be a clear and significant association between the presence of guns at home and suicidal ideation (for those that do not carry out suicide attempts). This result shows that more research has to be done to fully unveil the mechanisms that are driving suicidal ideation among adolescents. If supported by future research, the results could be highly important for policy makers, since they open up a range of possible interventions to improve mental health and reduce suicidal thoughts. More restrictive gun laws, for example, could indirectly reduce the odds of adolescents having suicidal thoughts.
Additionally, I have calculated the coefficient for “gun” in model 4 using the same logistic regression model but different methods of matching for the data. I have done this to test my results for robustness. For space reasons, I have placed the table in the Appendix (See 2. Coefficient of interest - different matching methods). The results obtained by model 4 are roughly consistent across the two additional methods of matching (“nearest” and “subclassification”) and can be replicated even without using matching (and even without imputing). All results are statistically significant at the 1% level. This means that, independently of the method of matching, we can observe roughly the same association between guns and suicidal ideation. This finding increases my confidence in my analysis and shows that the results obtained in Table 2 are robust to other methods of matching.
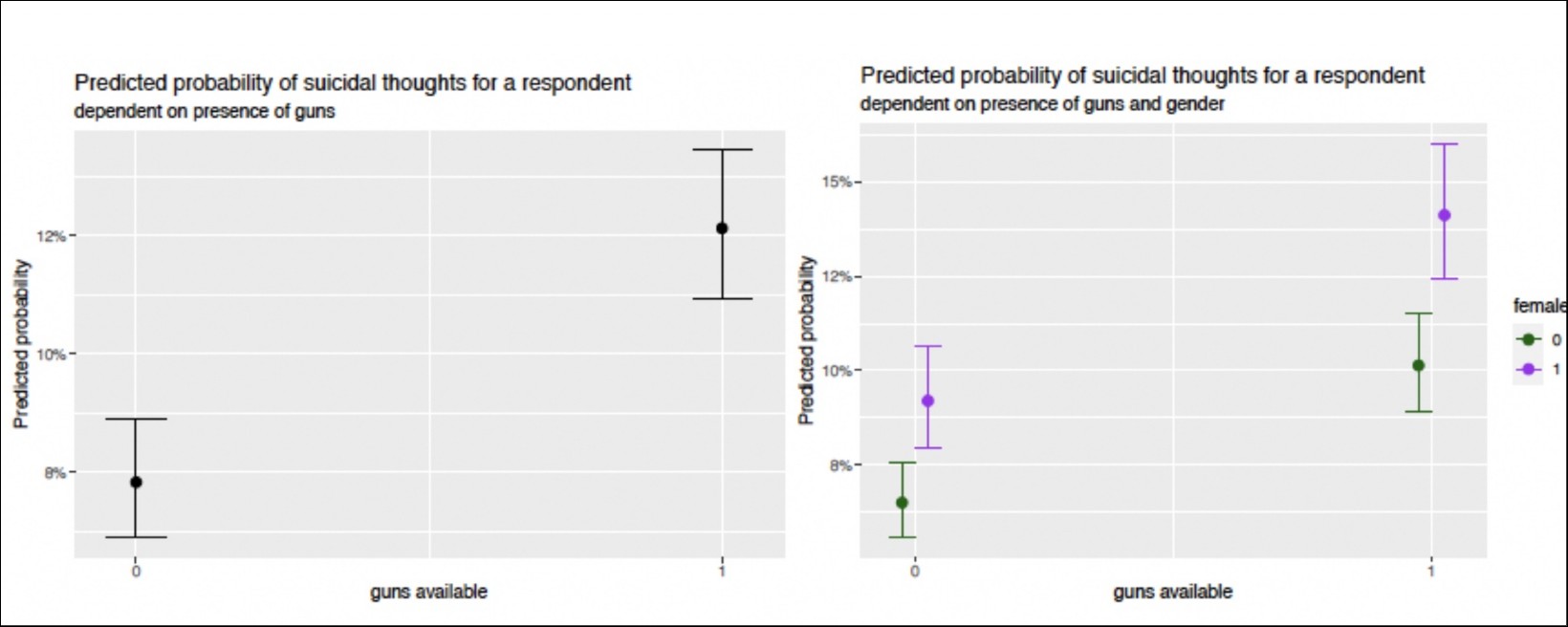
Below I provide two plots that I consider of some importance. The plot on the left shows the relationship between my key explanatory variable and the dependent variable. We can see how having guns is associated with an increase in the predicted probability for suicidal thoughts. This aligns with our results from Table 2.
{kind=link}
Additionally the plot on the right shows the relationship between gun ownership, gender and predicted probability for suicidal thoughts. I add this plot to show that the obtained results are consistent with prior literature and research on suicidal ideation. As has been shown by past research, while men tend to commit suicide more often, it is more common for females than males to actually have suicidal thoughts (Canetto and Sakinofsky, 1998). This can clearly be seen in the second plot. This second plot shows that the results obtained replicate common findings on suicidal indentation and add additional confidence to my results.
Discussion
In the following section I will review certain limitations to my findings and several threats to inference. As I have pointed out before, we are dealing with observational data. I, therefore refrain from making casual claims. To do so, randomized control trials should be conducted. However, in light of the topic, it seems unlikely that those will be performed at any point in time given they would be considered unethical. Moreover, since my analysis uses data from the mid-1990s my findings are only generalizeable to the general adolescent population in those and not to the current times. Since the 90s the American society has experienced many fundamental changes especially regarding technology and online infrastructure. Those changes gravely impact the generalizability to the present-day adolescent population since we can assume that the interviewed sample of adolescents for the Add Health data differs systematically from a random sample of adolescents in 2021. Additionally, I have to note that the results are not extendable to the adult population since the analysis was conducted on a sample of adolescents.
A shortfall of this analysis is that it doesn’t provide insight into which way a possible cause-and-effect relationship could go. I have refrained from making casual inferences since I am not performing a randomized control trial. Still, this analysis fails to answer whether having access to guns increases the risk of having suicidal thoughts or if people with suicidal ideation might just be more likely to get guns in order to eventually execute their plans. Since I am dealing with a sample of adolescents I assume that most did not own guns themselves but that the guns at home were simply bought by parents or guardians. This assumption would help to exclude the second interpretation. However, future researches should try to base this intuition on data in order to be able to make a grounded conclusion and solve this limitation.
Another important remark I want to make is that this analysis does not divide between certain types of guns such as handguns, shotguns or rifles. Past research has shown that not all firearms are equally likely to be used for suicide (Wintemute et al, 1988). Future analysis should, therefore, try and disentangle whether the association with suicidal indentation is the same for all firearm or whether there exist substantial differences between owners of different gun-types. I also want to highlight at this point that it is imaginable that, due to social stigma or simply fear, respondents systematically under-reported having suicidal thoughts. Since I am using self-reported numbers, we could have some bias in our numbers. This, however, is difficult to solve since there is no easy way to check whether respondents were truthfully answering questions. Another possible extensions to this analysis could include adding more important covariates such as data on geography, education and socioeconomic status, which could all potentially influence the results and cause omitted variable bias. Additionally, similar analysis should be conducted on representative samples of the adult American population in order to see whether the results obtained for teenagers can be extended beyond just their age group. This is important in order to gather more evidence and draw a more complete picture of the impact of gun ownership on mental health and suicidal ideation.
Conclusion
This analysis has provided evidence that the presence of guns at home could possibly be associated with an increase in suicidal ideation in adolescents. These results contradict the more prevalent school of thought which claims that although the presence of guns might be positively correlated with suicidal rates, it is not directly linked to increased suicidal thoughts. Future researches should consider this topic in more detail since it could have substantial influence on possible policy decisions concerning gun restriction laws.
References
Canetto, S.S., Sakinofsky, I. (1998). The Gender Paradox in Suicide. Suicide and Lifeâ€Threatening Behavior, 28, 1-23.
Ethan Heinzen, Jason Sinnwell, Elizabeth Atkinson, Tina Gunderson and Gregory Dougherty (2021). arsenal: An Arsenal of ‘R’ Functions for Large-Scale Statistical Summaries. R package version 3.6.2.
Hlavac, Marek (2018). stargazer: Well-Formatted Regression and Summary Statistics Tables. R package version 5.2.1.
Knopov, A., Sherman, R. J., Raifman, J. R., Larson, E., Siegel, M. B., (2019). Household Gun Ownership and Youth Suicide Rates at the State Level, 2005–2015. American Journal of Preventive Medicine, 56(3), 335-342.
Lester, D., (1989). Gun ownership and suicide in the United States. Psychological Medicine, 19, 519-521.
McCann, Stewart J. H., (2010). Suicide, Big Five Personality Factors, and Depression at the American State Level. Archives of Suicide Research, 14(4), 368-374.
Miller M., Barber C., Azrael D., (2009). Recent psychopathology, suicidal thoughts and suicide attempts in households with and without firearms: findings from the National Comorbidity Study Replication Injury Prevention, (15), 183-187.
Miller, M., Lippmann, S. J., Azrael, D., Hemenway, D., (2007). Household Firearm Ownership and Rates of Suicide Across the 50 United States. The Journal of Trauma: Injury, Infection, and Critical Care, 62(4), 1029-1035.
Simon, T. R., Swann, A. C., Powell, K.E., (2001). Characteristics of impulsive suicide attempts and attempters. Suicide and Life-Threatening Behavior, 32, 49–59.
Wintemute, G., Teret, S. P., Kraus, J. F., Wright, M. W. (1988). The Choice of Weapons in Firearm Suicides. American Journal of Public Health, 78, 824-826.
1.) This variable is called at_suicide in the Codebook. Aside from using it to filter out those that tried to kill themselves, this variable is not relevant to our analysis.
2.) “gun,” “age,” “female,” “race,” “health,” “religion,” “intelligence,” “abuse,” “psychological problems”
3.) Note: Since I have not imputed values for “suicide,” after the imputation procedure there is still some missingness in the data. I drop these few observations (about 60 out of over 5000 observations). I do this to simplify the matching procedure which will be conducted later. I do not expect this to be a problem since the percentage of observations dropped is extremely low.
4.) In other words: matching is conducted to be able to compare “apples-to-apples.” The idea behind propensity score matching is to use a linear combination of covariates to calculate one single value. In doing so, CBPS matching balances control and treatment group over a large spectrum of different covariates.
5.) See 5. Full summary statistics for summary statistics with different methods of matching that shows that CBPS does the best job.
6.) Please refer to the Appendix under 3. Covariate Balance before/after matching with CBPS for a covariate balance plot that shows how the matched data is better balanced than the unmatched data.
7.) See Appendix under 4. ANOVA tables for all tables regarding ANOVA tests
8.) See collinearity plot in the Appendix under 8. OLS collinearity check.
9.) See Appendix under 1. Full regression table for a table with the full set of covariates
10.) Note: The baseline categories for the covariates are: male (0) for “female,” 0 years for “age,” white (0) for “race,” moderately below average (0) for “intelligence,” poor (0) for “health,” none (0) for “religion,” no (0) for “substance abuse” and no (0) for “psychological problems.”